Beyond “How Much Do You Drink?”: A Structured Approach to Screening and Assessing Alcohol Use

Learning Objectives:
By the end of this article, the learner should be able to:
- Understand the importance of a comprehensive alcohol history in the diagnosis and evaluation of alcohol-associated liver disease
- Apply validated screening tools to identify harmful alcohol use
- Conduct and interpret a structured alcohol use history to quantify intake and characterize patterns of alcohol use
- Recognize clinical features suggestive of alcohol use disorder and incorporate DSM-5 criteria into assessment
The Basics of Alcohol-associated Liver Disease
Alcohol-associated liver disease (ALD) encompasses a spectrum of liver injury resulting from harmful alcohol use. This includes steatosis and steatohepatitis to more severe forms including acute alcohol-associated hepatitis (AAH), cirrhosis (AC) and the development of hepatocellular carcinoma (HCC). The quantity of alcohol ingested is the most important risk factor for the development of ALD, although the relationship is not strictly linear. Disease progression is dependent on continued excessive alcohol consumption, in addition to risk factors such as biological sex, genetic susceptibilities, tobacco use, diet, metabolic syndrome, and coexisting liver conditions.
Steatosis may develop in as little as two years of heavy alcohol use, whereas cirrhosis typically requires often a decade or more of sustained consumption above risk thresholds. Proposed threshold for diagnosing ALD is hepatic disease with an alcohol intake exceeding 350g/week in women and 420g/week in men in the absence of metabolic dysfunction. Lower thresholds apply in the presence of metabolic dysfunction, 140g/week in women and 210g/week (men), now recognized as metabolic dysfunction-associated ALD (MetALD). Understanding the amount and pattern of alcohol use is important in the diagnosis of AAH as the criteria includes excessive alcohol use for greater than 6 months with less than 60 days of abstinence.
ALD is differentiated from other causes of steatosis, fibrosis and cirrhosis through careful assessment of drinking history and exclusion of other causes of chronic liver disease. Elucidating the amount, duration and patterns of alcohol intake from the patient is crucial in informing the diagnosis and the risk of disease progression. The challenge of identifying harmful alcohol use and diagnosing ALD comes in part because alcohol histories are frequently inconsistent and underreported due to stigma and recall bias. Inconsistencies in drink sizes, global differences in “standard drink” definitions, and variable thresholds for biological sex and drinking patterns further complicate assessment. The remainder of this article will outline an approach to screen for alcohol use disorder and to obtain a structured, nonjudgemental and comprehensive drinking history. Check out other Liver Fellow Network articles on Biomarkers and treatment of alcohol use disorder (AUD)!
Screening for Harmful Alcohol Use
The AASLD and ACG recommend routine screening for alcohol use across all clinical settings. Screening in general medicine and specialty clinics has been shown to identify patients with ALD early, and structured and validated screening has been shown to effectively uncover harmful alcohol use compared to biochemical testing.
The AASLD recommends initial screening with the NIAAA single alcohol screening question (SASQ) for binge drinking or the three question Alcohol Use Disorders Inventory Test (AUDIT-C) (Figure 1). An AUDIT-C score of 4-5 has a high sensitivity (73-97% women, 82-100% men) and specificity (28-91% women, 34-89% men) for harmful alcohol use. Patients can then undergo a more detailed alcohol history and formal assessment for alcohol use disorder using DSM-5 diagnostic criteria (Table 1). The Alcohol Symptom Checklist may be used by providers or for patients to self-report the presence or absence of the 11 AUD symptoms defined by the DSM-5 (Figure 1).
Figure 1. An Approach to Alcohol Use Screening
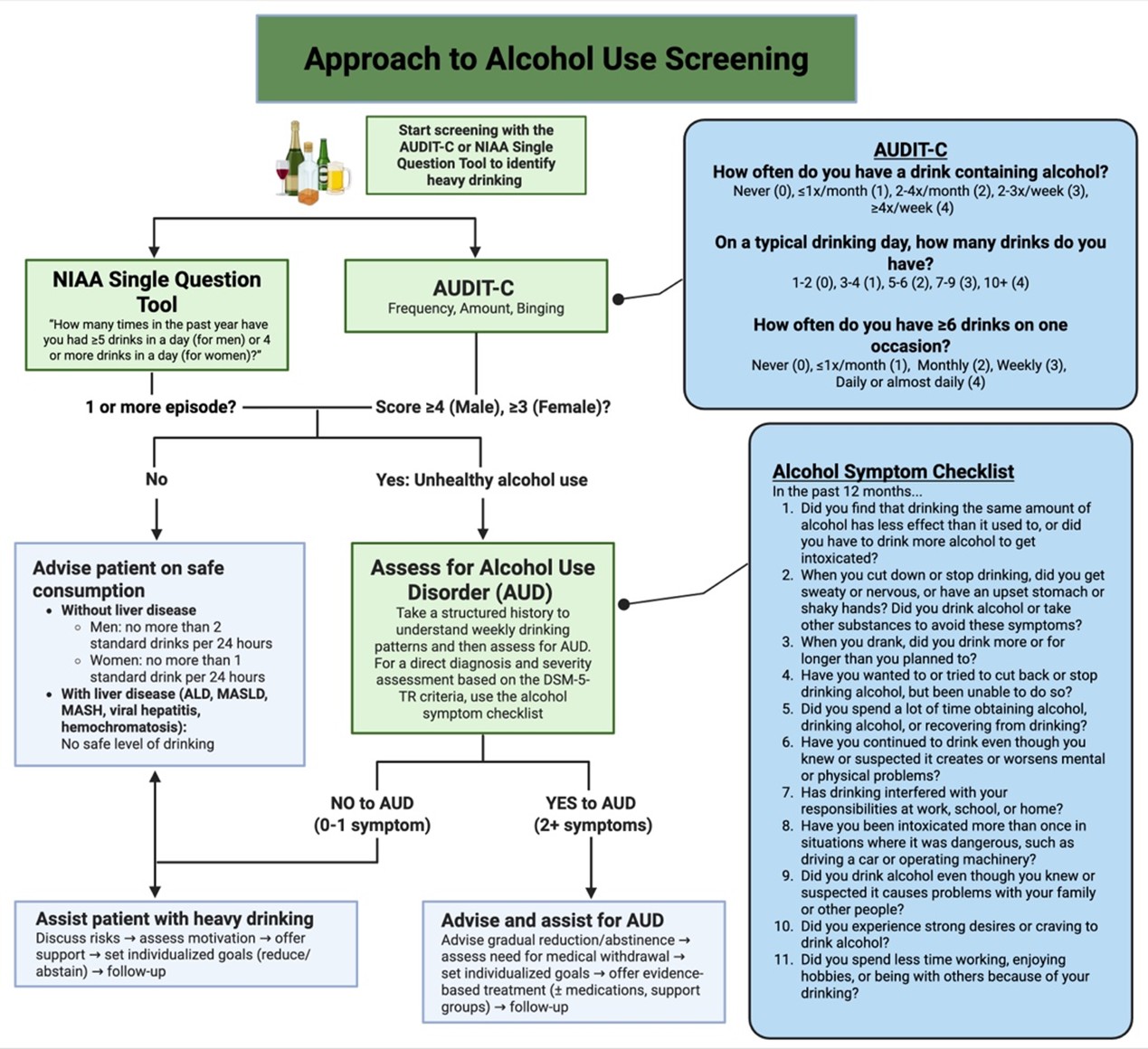
An Approach to Alcohol Use Screening. Created in BioRender. https://BioRender.com/y7vf20s
Conducting a Structured History
Once harmful alcohol use is identified, a detailed and structured history is essential. The way alcohol use is discussed can significantly influence the accuracy of patient reporting. Current guidelines from major hepatologysocieties have transitioned from the term “alcoholic liver disease” to “alcohol-associated liver disease” to promote stigma-conscious, patient-centered language. This approach should also inform the way an alcohol history is taken. Patients are prone to feeling judgement and guilt and may become defensive. A nonjudgemental, open and normalized interview style can reduce stigma and improve disclosure.
The alcohol drinking history should elicit the average quantity of alcohol consumed daily, the pattern of drinking relative to time and events and the impact of drinking on functioning, well-being, work and relationships. Rather than asking direct and confrontational questions such as “How much alcohol do you drink?”, clinicians should use a sequenced approach starting with frequency, then location and then quantity.
Frequency:
- How often do you drink any alcohol? (daily, weekly, monthly)
- Under what circumstances do you typically drink? (e.g. with meals, socially, special occasions, when stressed)
- At what age did you begin drinking?
Location:
- Where do you typically drink? (home, bars, social settings)
Quantity:
- What type of alcohol do you usually drink? (wine, beer, spirits/liquor)
- What kind of beer/wine/liquor do you drink?
- How much do you drink most days? (quantify in fluid ounces or liters)
- What is the maximum amount you consume at one time?
- How often do you purchase alcohol, and what/how much do you typically buy each time?
It is important to identify drinking patterns including binge drinking and drinking outside of mealtimes. Binge drinking is defined as consuming enough alcohol in a short period to raise blood alcohol concentration to at least 0.08%. This generally corresponds to about four or more drinks for women, or five or more drinks for men, within roughly two hours. Drinking outside of meals has been associated with a 2.7-fold increase in the risk of ALD compared to that who only consume alcohol at mealtimes. In addition to daily drinking, binge drinking has also been associated with increased risk of ALD and all-cause mortality.
Quantifying Intake
Estimating the amount of alcohol intake can be challenging. In the United States, a standard drink is defined as 14g ethanol which can be found in 5 oz wine, 12 oz regular beer, 8-9 oz of malt liquor and 1.5 oz of 80-proof spirits (“hard liquor”) (Figure 2). Note that 1 US fluid oz roughly equals 30 mL.
It is important to be aware of commonly used terms to describe quantities of liquor including “a pint” (16 oz), “a fifth” (25 oz) and “a handle” (59 oz) which can help improve accuracy. Online calculators can be used to translate reported drinking patterns into standardized drink units and to estimate total alcohol intake in grams.
Figure 2. Examples of one U.S. standard drink by alcohol type
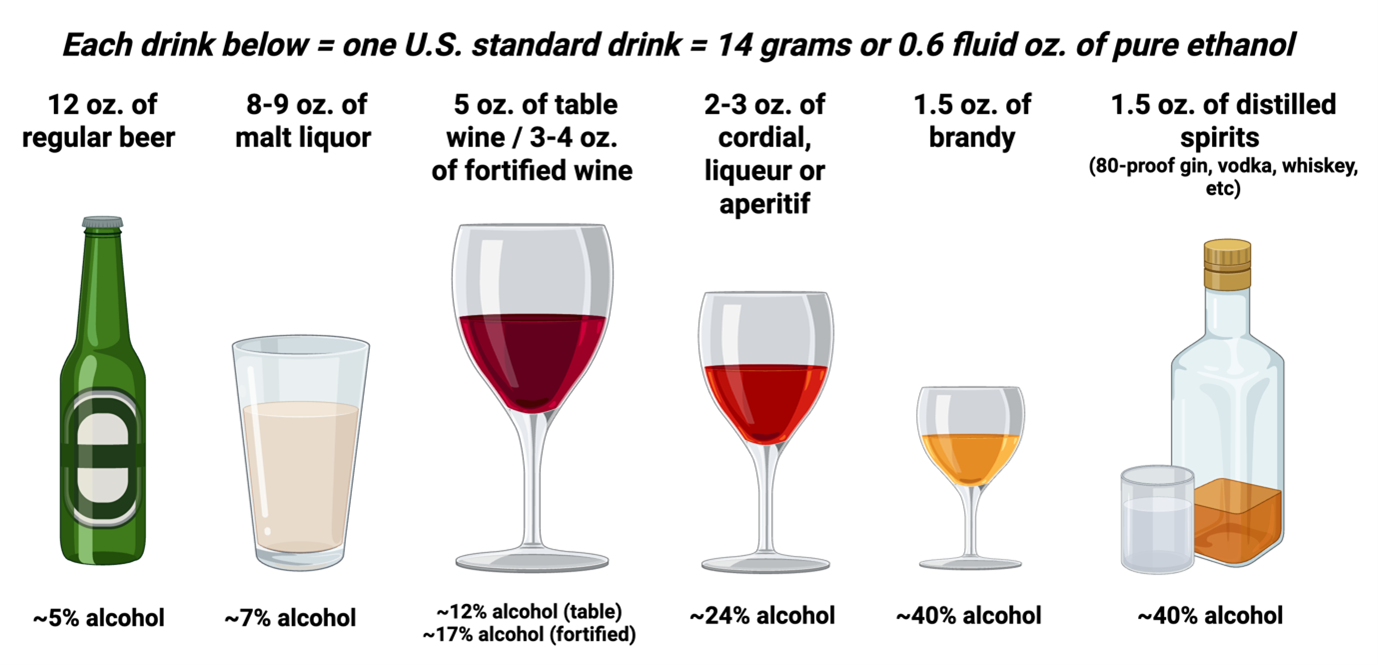
Examples of one U.S. standard drink by alcohol type. Created in BioRender. https://BioRender.com/bj5fd1r.
Figure adapted from: https://www.niaaa.nih.gov/alcohols-effects-health/what-standard-drink
Assessing for Alcohol Use Disorder and Clinical Impact
In addition to quantifying alcohol use, clinicians should assess the broader impact of alcohol on health and functioning.
It important to ask questions regarding interference with work/daily responsibilities, attempts to reduce or abstain from drinking, previous abstinences, cravings, tolerance and withdrawals. These domains align with the DSM-5 criteria for AUD and the Alcohol A ‘Symptom Checklist’ (Figure 1) can be used to guide formal diagnosis of AUD (Table 1).
Examples of key questions:
- Has drinking interfered with ability to attend, or responsibilities at missed work/school or home?
- Have you wanted or tried to cut back or stop, but been unable to do so?
- Have you ever successfully stopped drinking and if so, for how long?
- Do you experience strong desire or craving to drink alcohol?
- Do you find that drinking the same amount of alcohol has less effect that it used to?
- When you cut down or stop drinking do you experience sweating, nervousness, upset stomach or shaky hands?
Finally, given the genetic predisposition to both ALD and AUD, a family history of excessive alcohol use should also be obtained.
Table 1. DSM-V Criteria for Alcohol Use Disorder
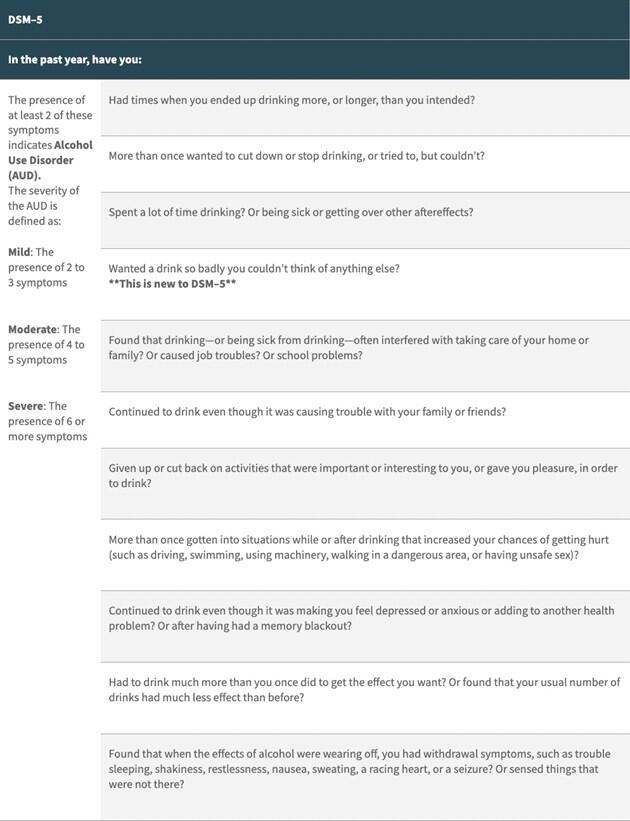
Table from: https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/alcohol-use-disorder-comparison-between-dsm
Take Home Points:
- A structured alcohol history is essential for diagnosing ALD, as accurate assessment of amount, duration, and pattern of use is critical to distinguishing ALD from other causes of liver disease and estimating risk of progression.
- Validated screening tools (SASQ, AUDIT-C) should be used routinely to identify harmful alcohol use, but positive results should always be followed by a more detailed, structured alcohol history.
- Quantifying alcohol intake using standard drink definitions improves accuracy and consistency, allowing for more reliable assessment of risk and clearer communication across providers.
- Patterns of alcohol use, including daily intake, binge drinking, and recent consumption, provide important diagnostic and prognostic information beyond total alcohol quantity alone.
- Alcohol use is frequently under-reported, and a nonjudgmental, structured approach improves disclosure and diagnostic accuracy, often making clinical history more informative than biomarkers alone
Written by:
Michael Gianarakis, M.D.
Internal Medicine Resident, University of Illinois Chicago
Reviewed by:
Vinay Jahagirdar, M.D. (Fellow Lead)
Bilal Khalid, M.D. (Faculty Editor)