Medical Therapies in Alagille Syndrome

Continuing on with our spotlight on Alagille syndrome, we will learn about medical management of Alagille and a newer class of medications, IBAT inhibitors. We will review the ICONIC trial, and below you'll find a review of medical management in Alagille syndrome (continuation of post by Kanak Verma).
Management of Alagille Syndrome
Medical
Pruritus
Intractable pruritus can significantly impact quality of life. Initial measures to minimize itching and subsequent excoriations include frequent nail cutting, skin emollients, and avoiding bathes in hot water. Off-label therapy options for pruritus include:
Table 2: Off-label medical therapy for pruritus
|
Medication |
Mechanism |
|
Ursodeoxycholic acid (UDCA, or ursodiol) |
choleretic, stimulates bile flow |
|
Cholestyramine, colesevelam |
bile acid-binding resins |
|
Antihistamines |
can help with poor sleep secondary to pruritus |
|
Naltrexone |
opioid receptor antagonist |
|
Rifampin |
exact mechanism unknown, likely pregnane X receptor (PXR)-agonist mediating downregulation of autotaxin transcription7 (autotaxin levels are markedly elevated in cholestatic pruritus and correlate with itchy intensity) |
When medical therapy fails, surgical biliary diversion or ileal resection can be considered prior to liver transplantation.
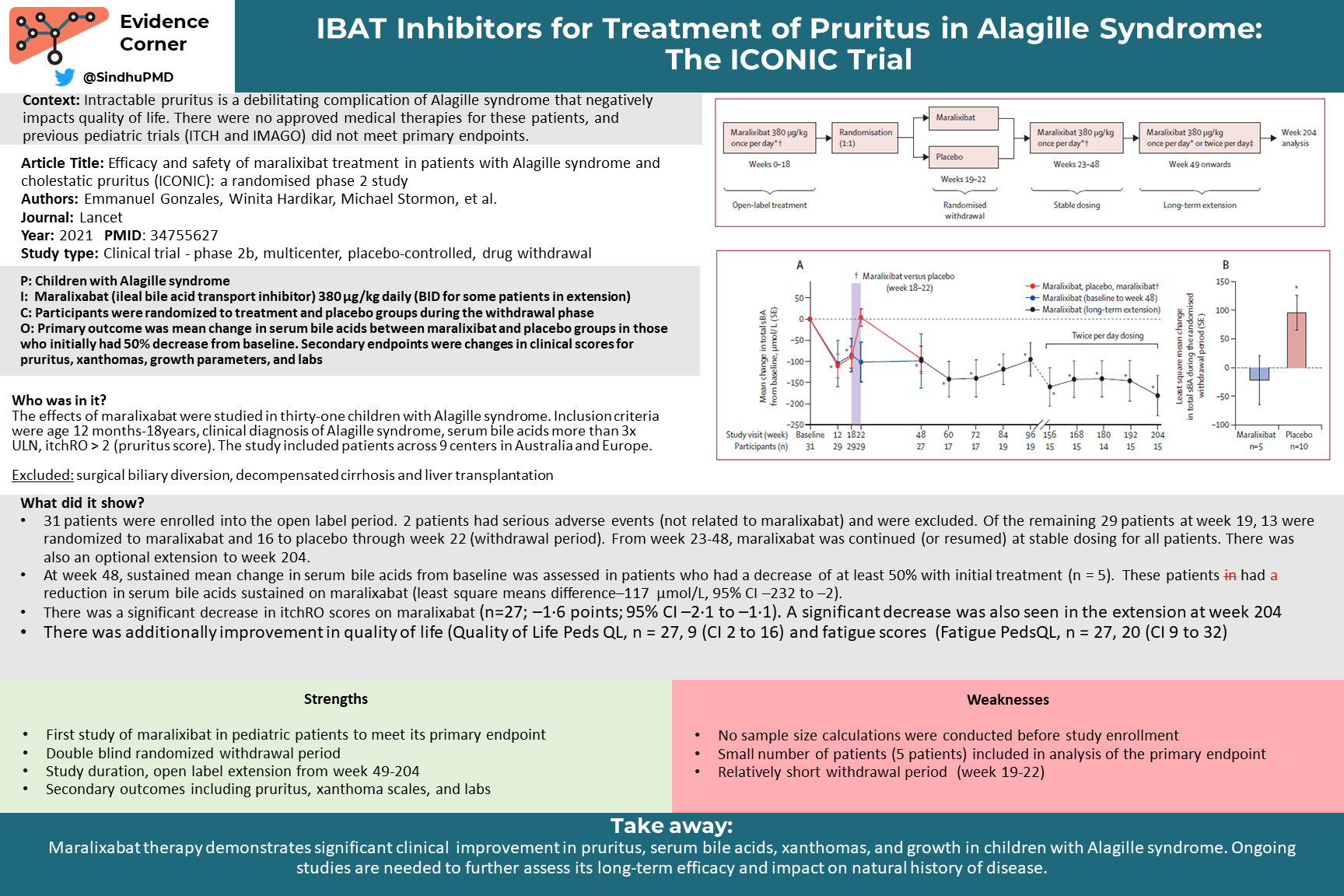
Ileal bile acid transporter (IBAT) inhibitors, including maralixibat and odevixibat, are a new class of medications used for the treatment of pruritus in cholestatic disease. These drugs act by interrupting enterohepatic circulation of bile acids (effectively serving as a “medical biliary diversion”). Clinical trials have demonstrated significant decrease in serum bile acids with associated clinical improvement in pruritus, xanthomas, and overall growth. Maralixibat (Livmarli) was recently approved in September 2021 for use in the treatment of cholestatic pruritus in patients 1 year of age or older with Alagille syndrome.5 Odevixibat (Bylvay) is currently approved for patients 3 months of age or older with progressive familial intrahepatic cholestasis (PFIC), and there is currently a Phase 3 clinical trial ongoing for patients with Alagille syndrome (NCT04674761).
Xanthomas
Xanthomas typically form when serum cholesterol levels exceed 500 mg/dL, and typically resolve with improvement in cholestasis. Of note, hypercholesterolemia from Alagille syndrome is largely associated with lipoprotein-X, a low-density lipid that is rich in phospholipids, albumin, and free cholesterol. Lipoprotein-X is not thought to atherogenic, therefore the hypercholesterolemia in Alagille syndrome is not associated with increased risk of cardiovascular disease and does not require dietary modifications or medical therapy. Statins have reportedly been used in severe debilitating cases (for example, where xanthoma interfere with functioning), and can have beneficial effect but have not been studied for this indication in children.6
Nutritional status
High-calorie supplements and nasogastric/gastric tube feeding may be necessary to provide adequate caloric intake for growth. Fat-soluble vitamin levels should be monitored routinely and supplemented as needed.
Liver transplantation
Survival to early adulthood with native liver occurs in approximately 24% of children. Typical indications for liver transplant in Alagille syndrome include intractable pruritus, liver synthetic dysfunction, portal hypertension, metabolic bone disease and fractures, and growth failure. Patients should undergo a complete cardiac and renal evaluation prior to transplantation, as underlying disease may impact post-transplant course and choice of immunosuppression regimen. Head imaging should also be obtained to assess for vascular anomalies that may impact bleeding risk.