Pathology Pearls: Intrahepatic Cholangiocarcinoma

Brief Case Presentation
A 73 year old female with past medical history of GERD, anxiety, asthma, and osteoarthritis presented with dark stools and abdominal distention.She was referred to gastroenterology for further evaluation. Laboratory tests were as follows and CT abdomen showed a 1.8 cm mass in liver segment IVb. A targeted biopsy of the mass is performed.
Selected lab values are as follows:
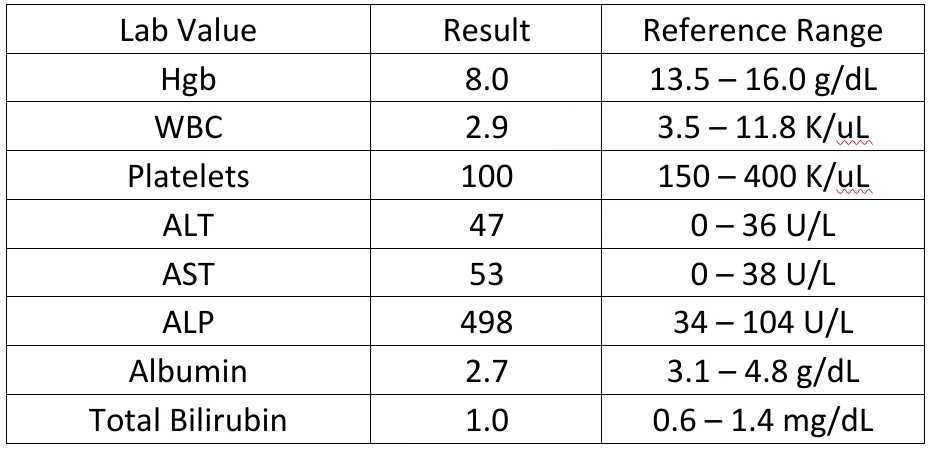
Liver biopsy findings
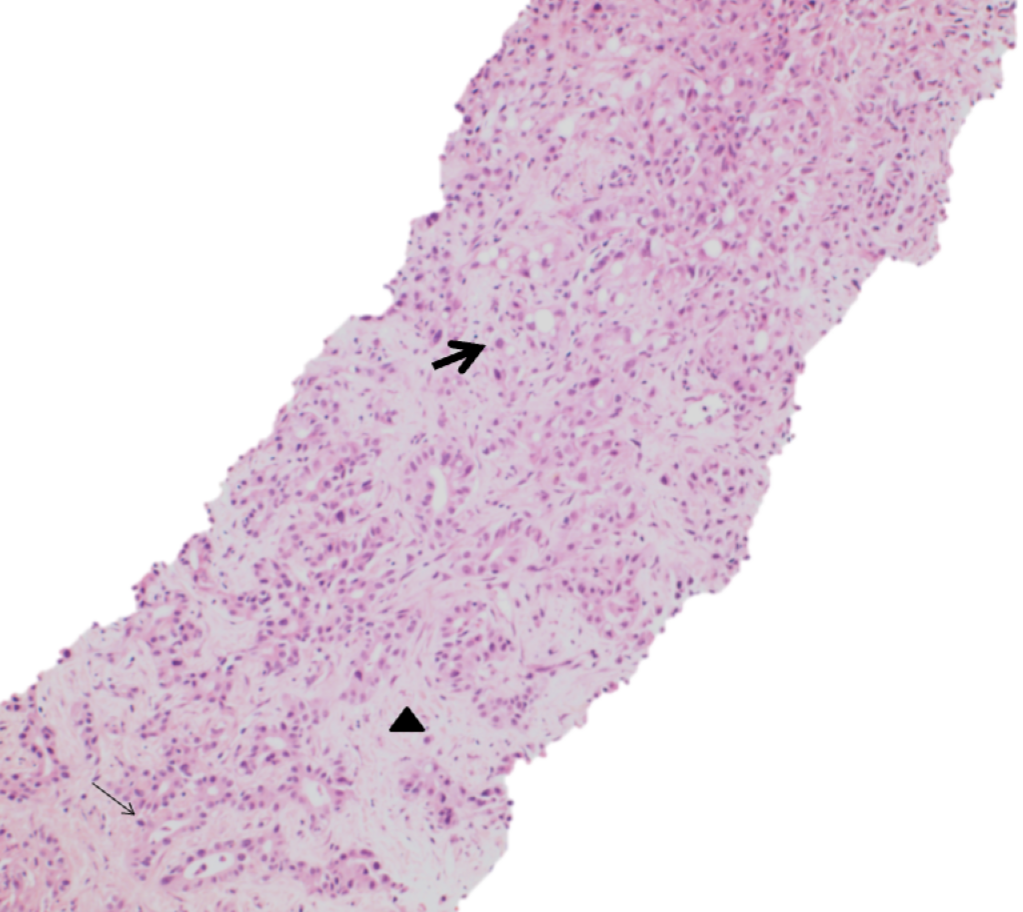
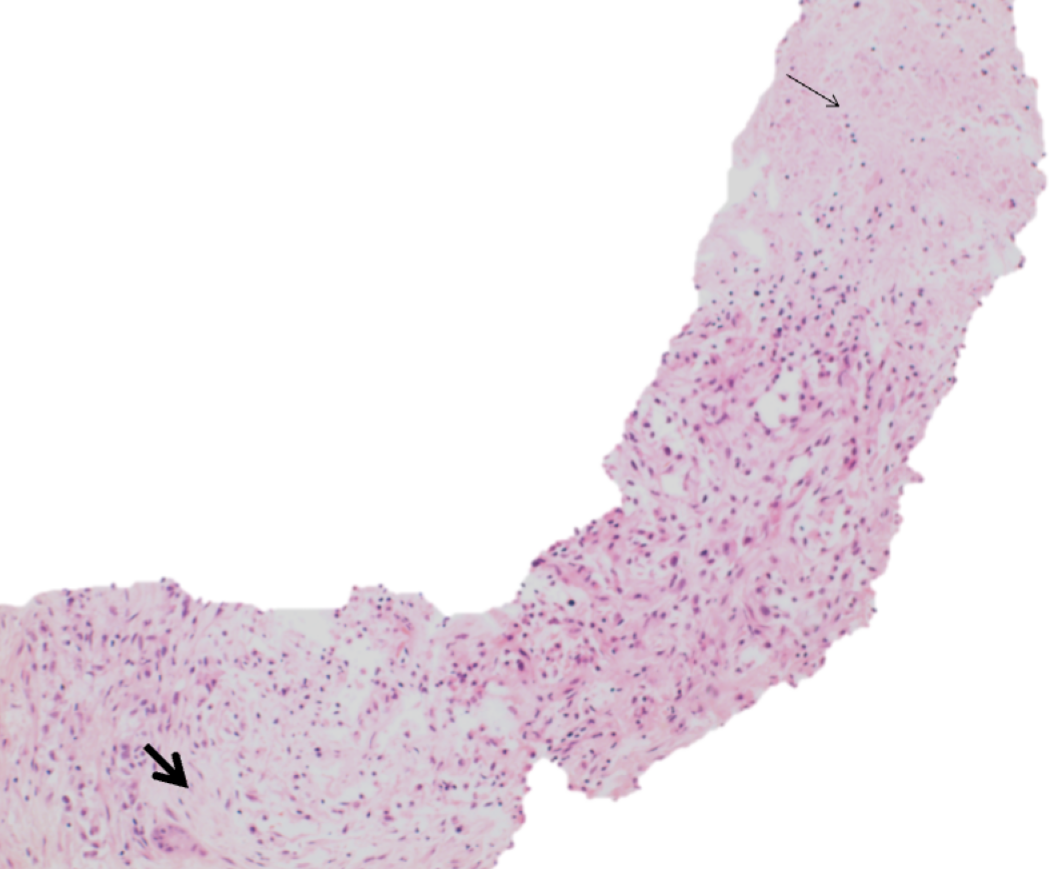
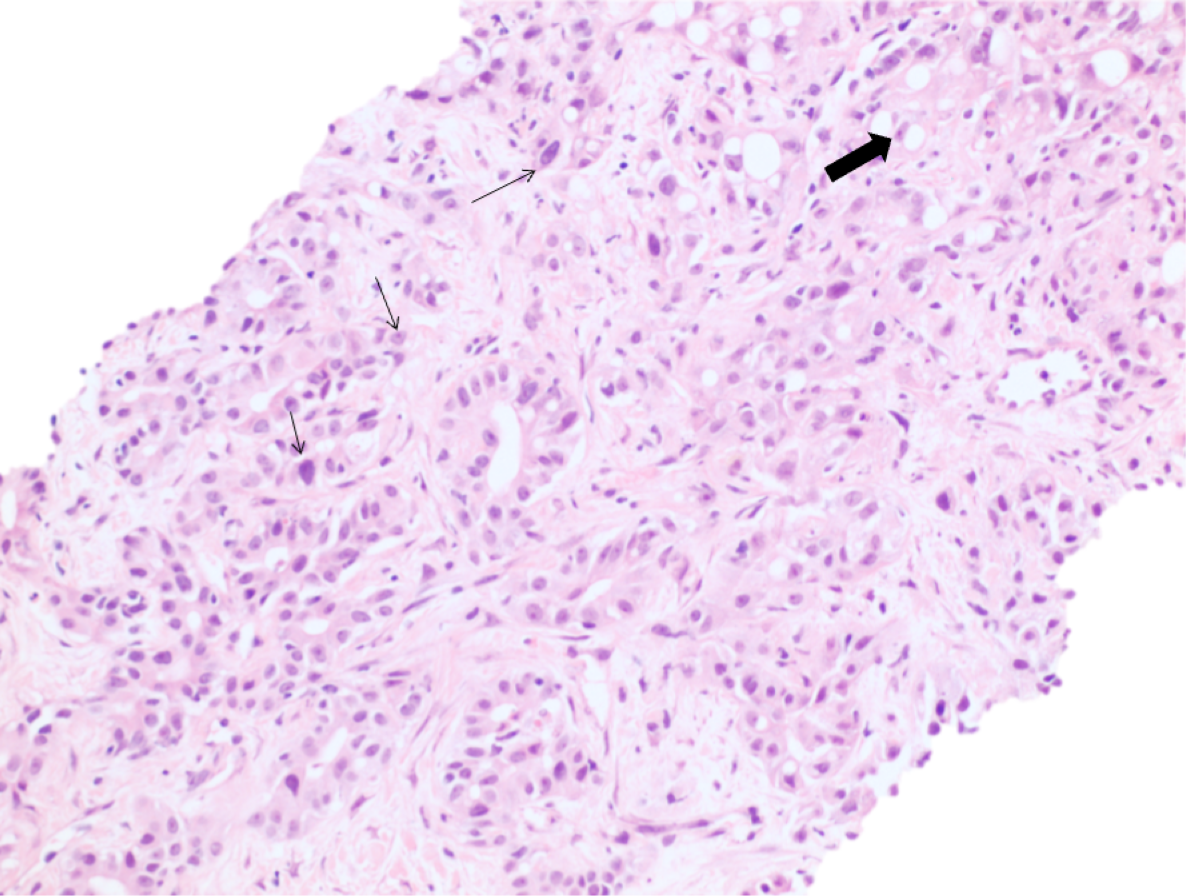
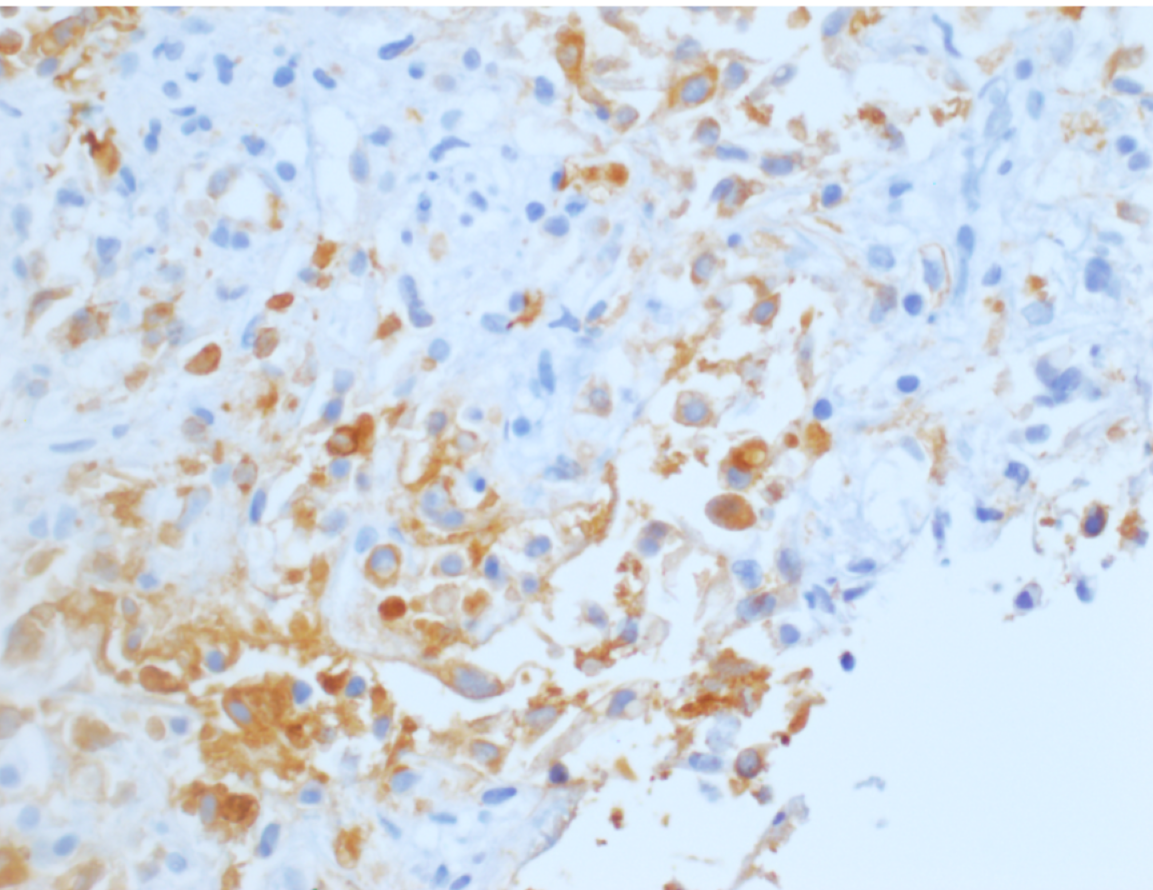
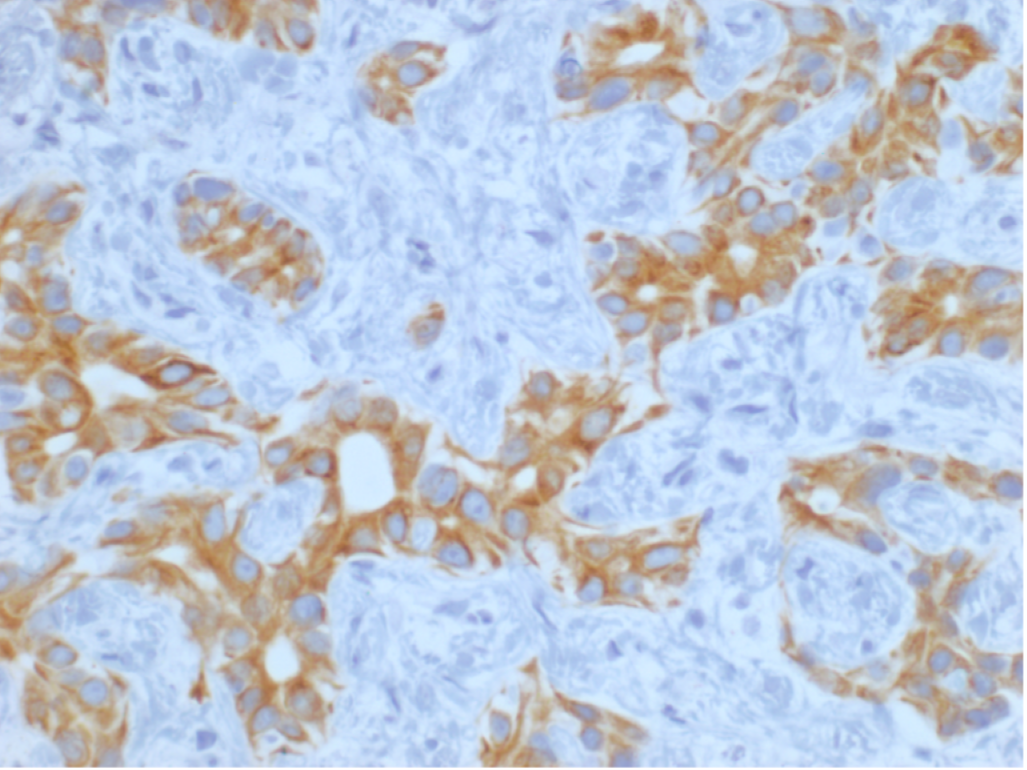
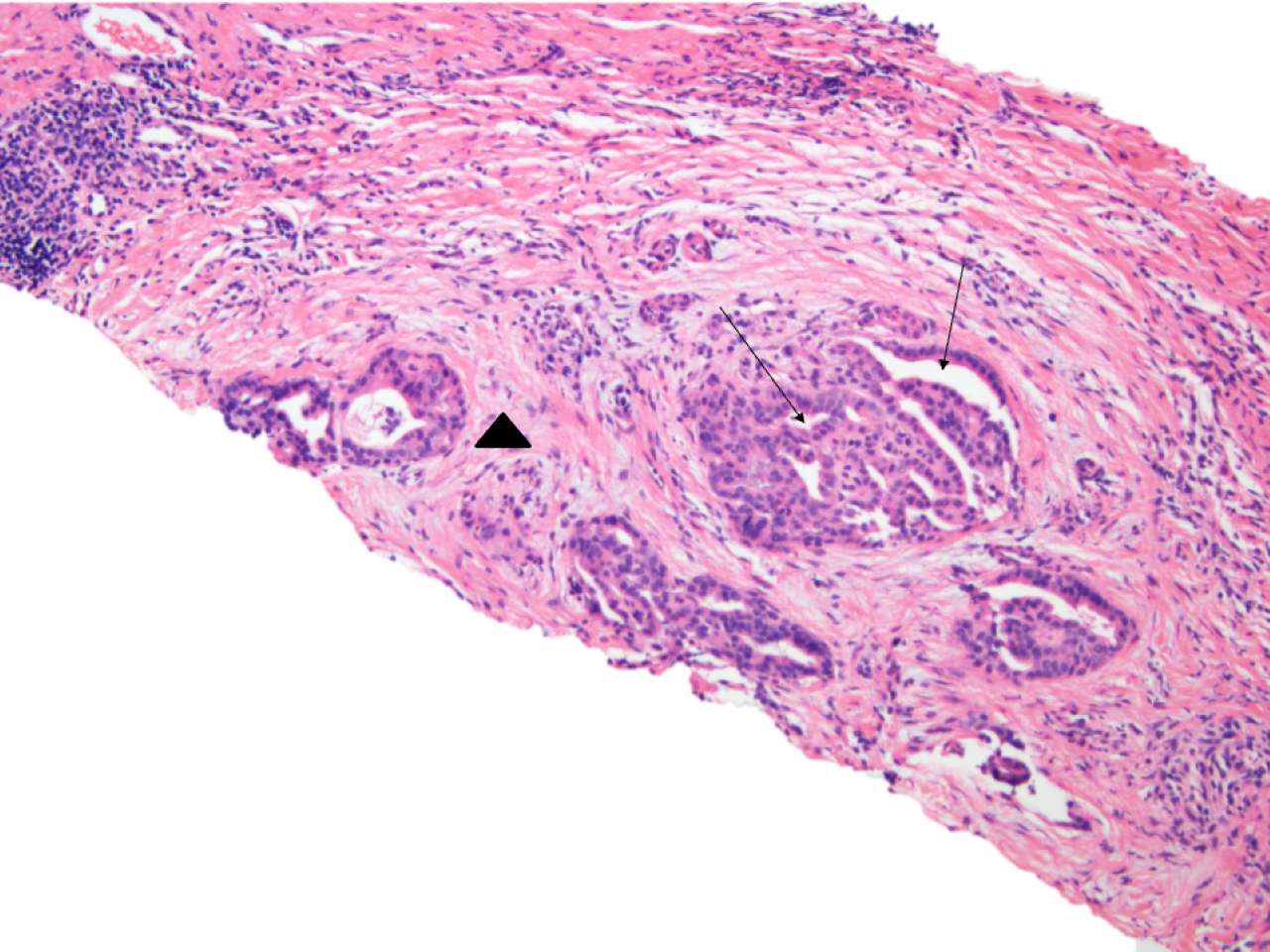
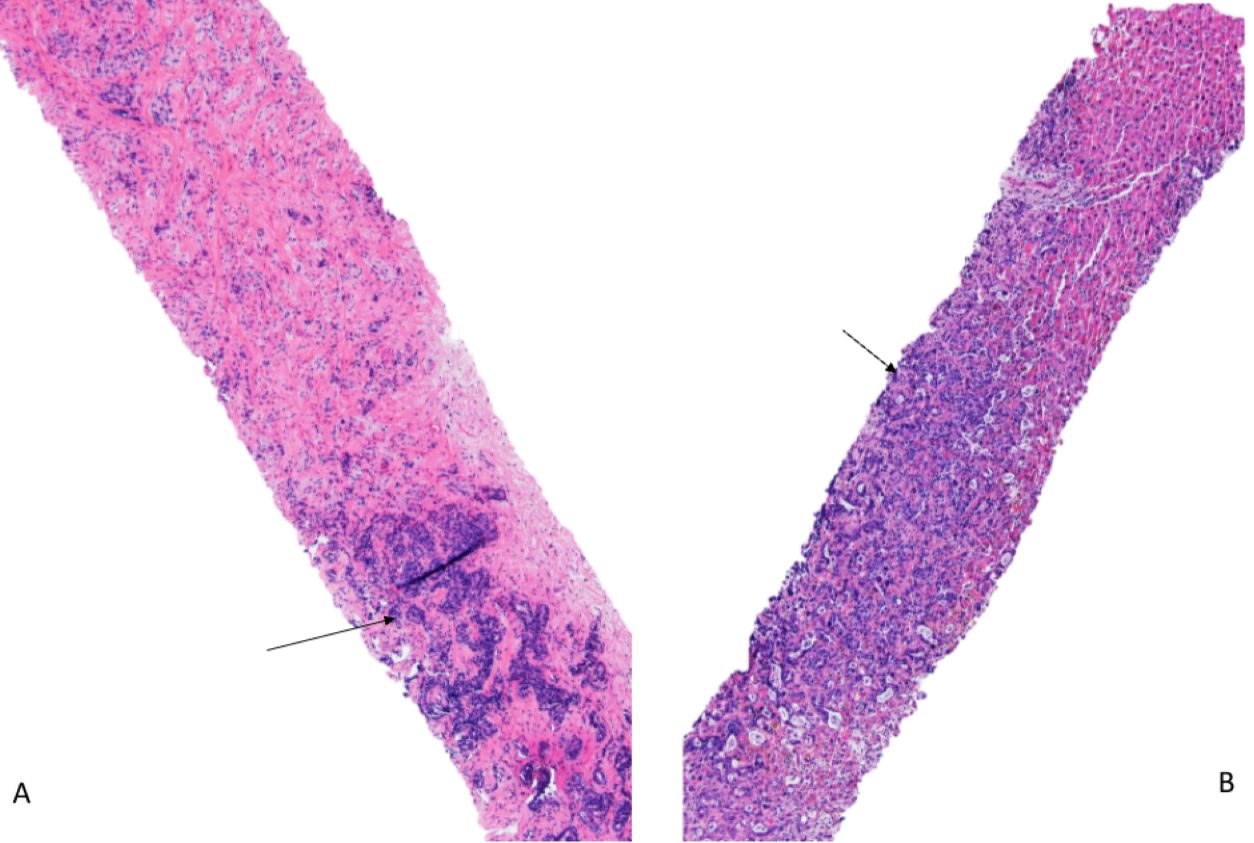
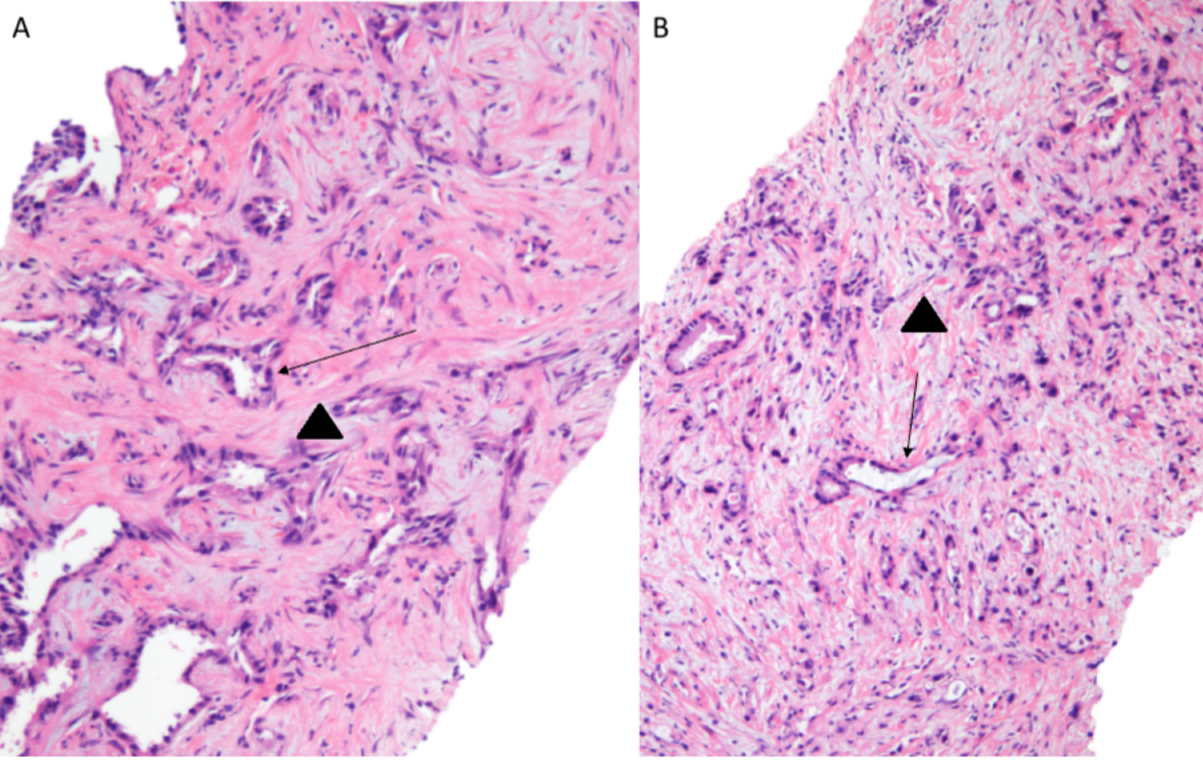
At low power, the liver core shows irregular angulated glands and single cells in a background of abundant desmoplastic stroma. (Figure 1 and 2). At high power the cells display varying degrees of cytologic atypia (Figure 3), consistent with a moderate to poorly differentiated adenocarcinoma. Immunohistochemical stains for CK7 (Figure 4) and CK19 (Figure 5) are positive. Immunohistochemical stains for Glypican-3, Arginase-1, CK20, GATA3, PAX-8 and CDX-2 are negative. In the clinical context of a single central intrahepatic lesion with absence of lesions in the rest of the body, the histologic findings are compatible with intrahepatic cholangiocarcinoma.
Cholangiocarcinoma
Cholangiocarcinomas are divided into extrahepatic, intrahepatic and hilar based on their location. The average age at diagnosis is >50 years with a slight male predominance. CA19-9 is typically elevated. Intrahepatic cholangiocarcinoma is the second most common primary hepatic malignancy after hepatocellular carcinoma. Its incidence is highest in south-eastern Asia especially Thailand.
Intrahepatic cholangiocarcinomas (iCCA) arise peripheral/proximal to left and right hepatic ducts. Risk factors include:
- Biliary tract inflammation and infection
- Liver Fluke infection
- Primary sclerosing cholangitis
- Hepatolithiasis
- Biliary tract malformation
- Caroli disease
- Congenital hepatic fibrosis
- Bile duct cysts
- Viral infection
- Hepatitis virus (HBV and HCV) infection
- Non-biliary cirrhosis
- Alcoholic liver diseases
- Hemochromatosis
- Metabolic syndrome
- Diabetes and obesity
- Chemical exposure
- Thorotrast
- Asbestos
- Occupational exposure to 1,2-dichloropropane and dichloromethane
- Smoking
Histologic features of Cholangiocarcinoma
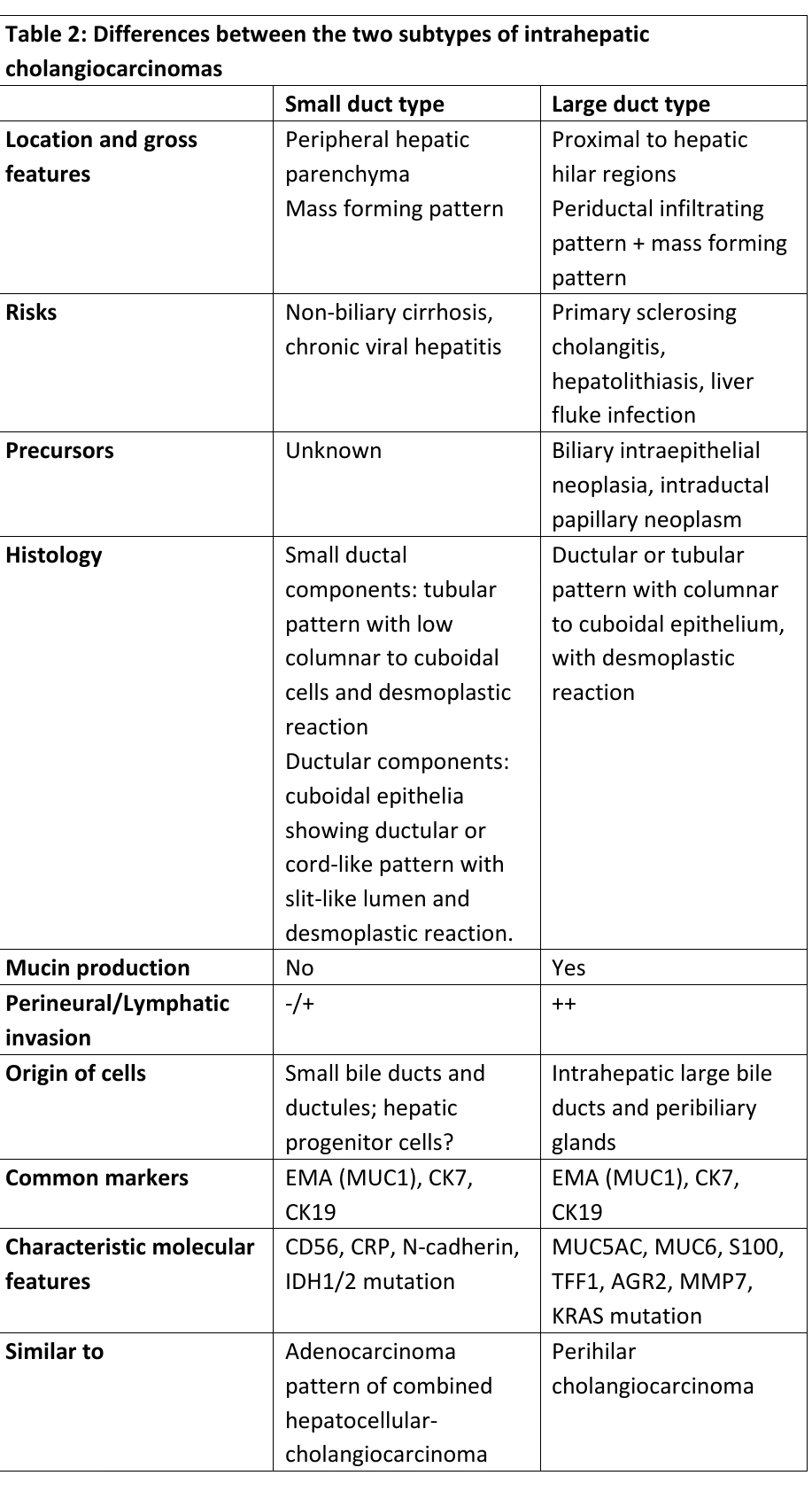
There are two main subtypes of iCCAs; small duct type (Figuure 6 and 7) and large duct type. Table 2 highlights the differences between the two types.
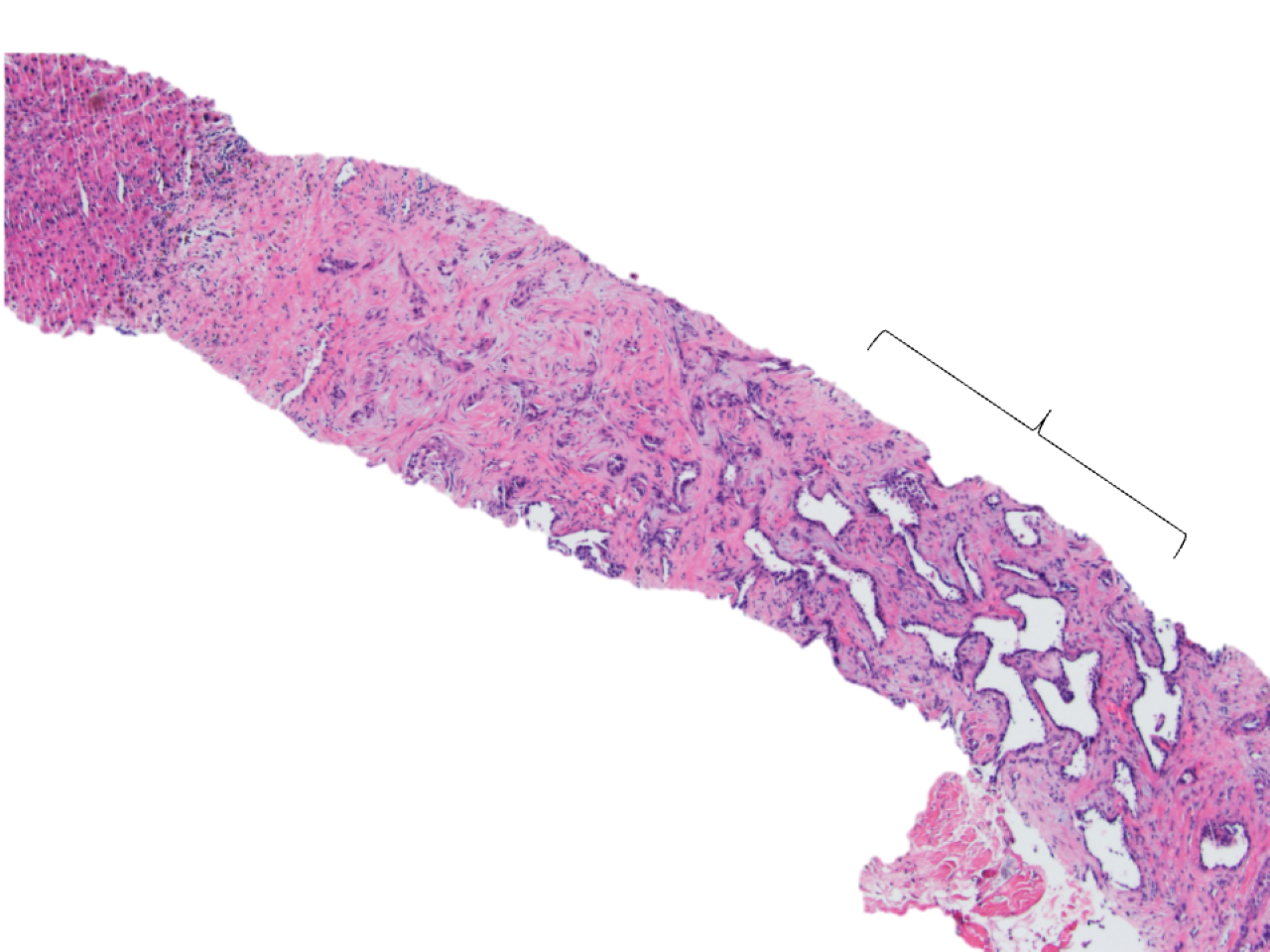
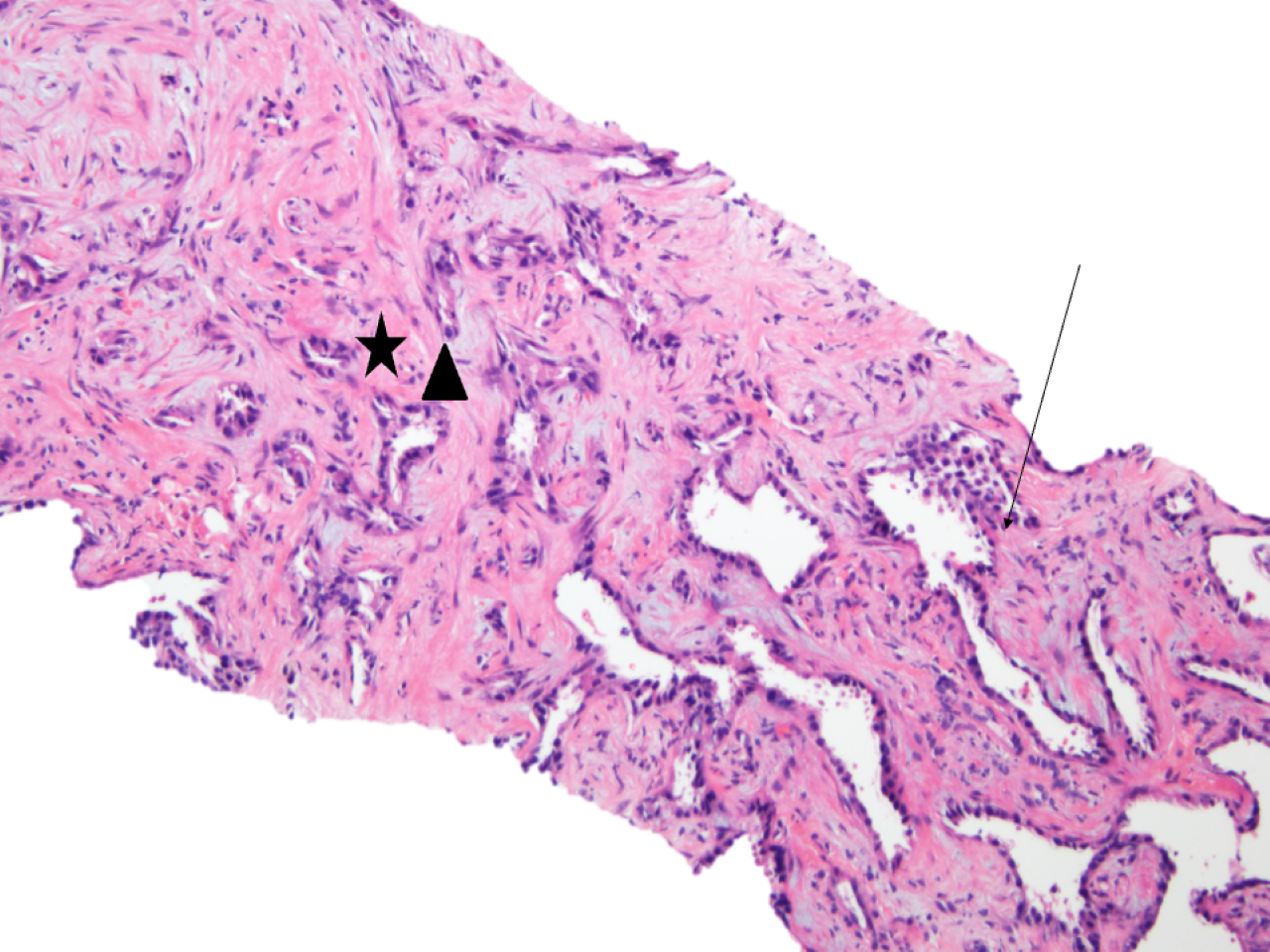
ICCAs are exclusively adenocarcinomas (Figure 8) with ductal or tubular pattern showing variably sized lumen. Some cases display a cord like pattern with slit-like lumen or a micropapillary pattern. The stroma in these cases is fibrous. The epithelium can be cuboidal or columnar with a variety of cell sizes ranging from small to large and pleomorphic. The cytoplasm ranges from eosinophilic to clear. Mucus secretion is more common in small duct iCCA and less so in large duct types.
Grading of intrahepatic cholangiocarcinomas is based on morphology:
- Well-differentiated: composed of well-formed glands
- Moderately differentiated: A mix of well and poorly differentiated features
- Poorly differentiated: composed of single cells or sheets of cells
Differential Diagnosis of Intrahepatic Cholangiocarcinoma
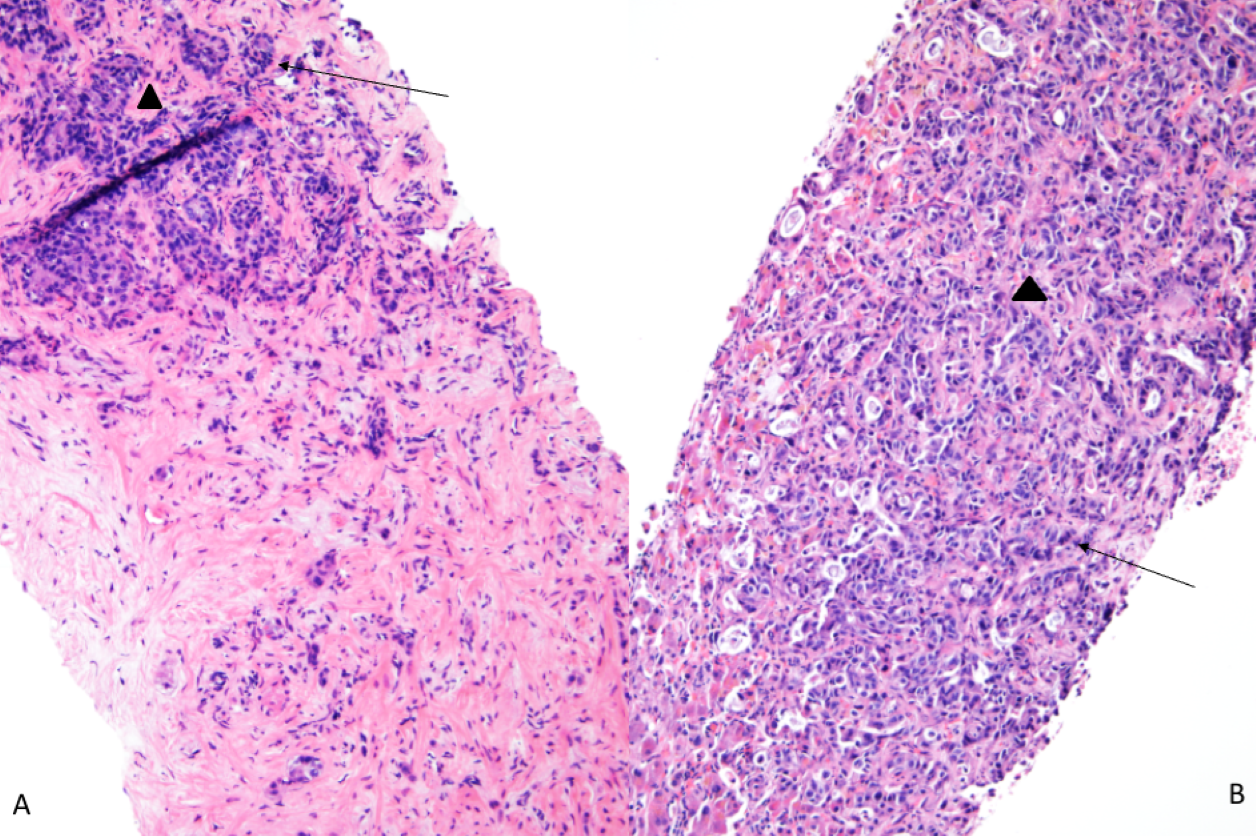
The main differential diagnoses include metastatic tumors from other parts of the gastrointestinal tract or the rest of the body as well as hepatocellular carcinomas (HCCs). The major question arises in the differentiation of intrahepatic cholangiocarcinoma from metastatic pancreatic adenocarcinoma. The histological features and immunohistochemistry for both are similar. Figure 9, 10 and 11 highlight the histological similarities between the two. The immunohistochemical profile for both is similar however, Albumin-ish is positive in iCCAs and negative in pancreatic tumors. Loss of BAP1 favors iCCAs versus pancreatic. A complete correlation of clinical history, radiological findings, histopathologic and immunohistochemical features is the most helpful thing in such cases.
A panel of immunohistochemical stains should be used to differentiate intrahepatic cholangiocarcinomas from other differentials as follows:
- Favoring Hepatocellular:
- Alpha feto protein
- Arginase
- Hep par1
- Glypican3
- Favoring cholangiocarcinoma:
- MOC-31
- CA19-9
- Cytokeratin stains show considerable overlap between hepatocellular and cholangiocarcinoma; CAM5.2 (CK8/18) is positive in both intrahepatic cholangiocarcinomas as well as HCCs however HCCs would be negative for other keratins. CK7 (90%) and CK19 (80 to 90%) are positive in most cholangiocarcinomas and CK20 can be positive in peripherally located cholangiocarcinomas.
- CDX2 can be positive in 40% of cholangiocarcinomas (a major pitfall to remember when differentiating cholangiocarcinomas from metastatic gastrointestinal tract tumors).
- TTF-1 and Napsin can be positive in hilar cholangiocarcinomas (a pitfall to remember when differentiating from metastatic lung adenocarcinomas)
- Other immunohistochemical stains for metastatic tumors include:
- Neuroendocrine: Synaptophysin, chromogranin (these would be positive in primary liver neuroendocrine tumors too so radiological findings help)
- Renal, müllerian: PAX8
- Breast: GATA3, Mammoglobin, GCDFP15
- Squamous: P40, CK5/6
- Urothelial: GATA3, P40, P63
- Adrenal: Mel-A, inhibin
- Mesothelial: WT-1, Calretinin, D240
- Pancreatic acinar cell carcinoma: Trypsin, BCL10
- Melanoma: SOX10, Melan-A, HMB-45
- Thyroid: TTF-1, Thyroglobulin
References
- Torbenson, Atlas of Liver Pathology: A Pattern-Based Approach. 2019
- Burt, MacSween’s Pathology of the Liver: Seventh Edition. 2017.
- WHO Classification of Tumors of the Digestive System, 5th ed. Lyon: IARC Press; 2019.