Why do we use living donors for liver transplantation?


Living donor liver transplant (LDLT) has now existed for decades and has saved hundreds of lives each year in the United States.
Have you ever wondered how it came about? Well, fasten your seat belts and join us for the ride!
When was the first LDLT performed in the US?
When Alyssa Smith was 11 months old, she was diagnosed with biliary atresia. Biliary atresia is a life-threatening pediatric progressive cholangiopathy that used to be a uniformly fatal diagnosis prior to the advent of the hepatoportoenterostomy (Kasai) surgery in the 1950’s. Even in patients who undergo Kasai surgery, survival with native liver ranges from 30-55% at 5 years, 30-40% at 10 years and ~20% at 20 years. Therefore, up to 80% of patients with biliary atresia will need a LT by adulthood. With a LT, most will live into adulthood. Prior to LDLT, patients diagnosed with this condition would have to wait for an available, good quality deceased organ to be available prior to transplantation. Alyssa’s family, however, was offered a unique opportunity at the University of Chicago whereby Alyssa’s mother could donate part of her liver to save her daughter’s life. Alyssa’s surgery was successful, and she is now over 30-years old with several children of her own.


We reached out to her to answer some questions and she was so kind to reply!
Q: How does it feel to be the recipient of the first ever living liver donation?
To be honest I knew I had the first living related liver transplant in the US but it was just normal life for me. My parents strived to give me and my brother a normal life. We sometimes forget people don’t know and then when I randomly make a comment people are like what??? And then I remember I forgot to tell that person.
Q: Tell us what your life is like now? Are you still on immunosuppression? Have there been any long-term sequelae from your surgery?
My life is pretty normal. I am not on any medication for my transplant at all. I have never had any issues with my liver. I had labs drawn all through my pregnancies and never showed any signs of anything. I have two wonderful children (4 years old and 1.5 years old) and stay at home. We have a pretty normal Midwest life!
Q: What advice would you give to people thinking about being a living donor?
I fully support any organ donation and have done many drives to get people to sign up to be donors. I believe it can be a hard decision, but it can be the most important decision for you and the recipient. I hope that others can see how it can change someone’s life to give a small gift. It is a small gift, but it means so much to others.
What is the history behind LDLT?
When LDLT was beginning, other centers learned about LDLT techniques by visiting the University of Chicago and observing, by hiring physicians trained in Chicago, and by independently developing protocols. Dr. Abhinav Humar, who is now the chief of transplantation at the University of Pittsburgh Medical Center (UPMC), learned by developing his own protocols at the University of Minnesota Medical Center. Now, UPMC performs greater than 50 living donor liver transplants per year.
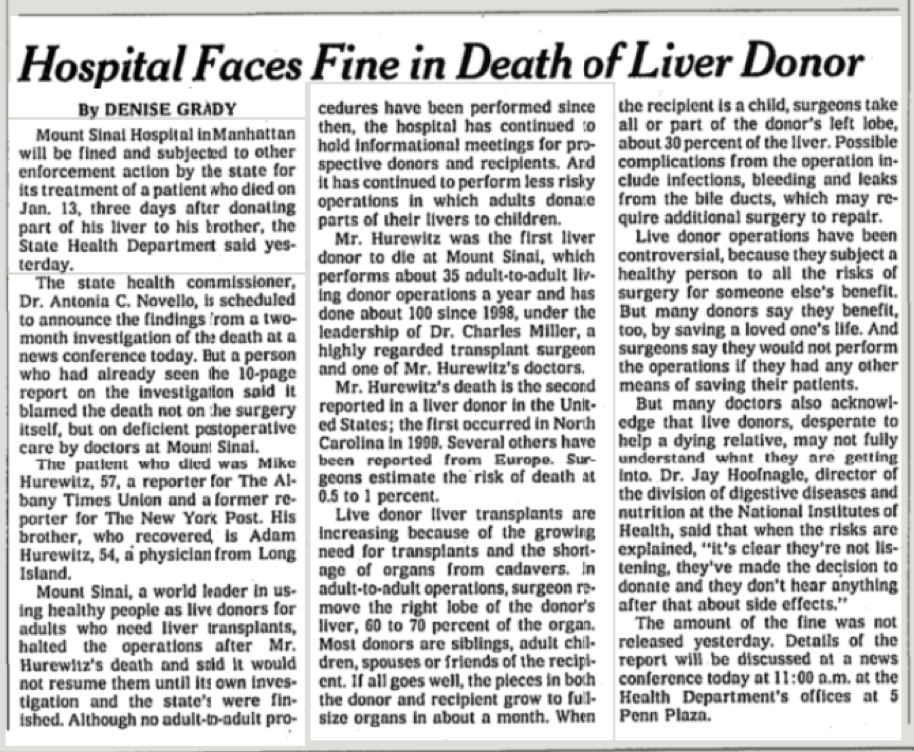
After successful LDLT in the pediatric population, surgeons began to apply the techniques they had learned to adults. In fact, in Asia, LDLT became (and still is) the predominant method of transplantation given the relative lack of deceased organs secondary to cultural factors and preferences. In the United States, the first adult LDLTs took place in the mid-90s, though they involved the transplant of only left lateral segments, which is safer for the donor. However, because many left lateral segments are too small for adult recipients, eventually, the transplant of right liver lobes began. The very first right lobe LDLT took place in 1997 with Wachs and his colleagues. By 2000, over 250 total LDLTs were performed at over 38 centers. The numbers of LDLTs rose steadily each year, until about 2001, at which point there was a decline. One of the proposed reasons for this decline was that there were several highly publicized donor deaths, though it is difficult to know if this was the only reason for the decline. One particular donor death was published in the New York Times, below:
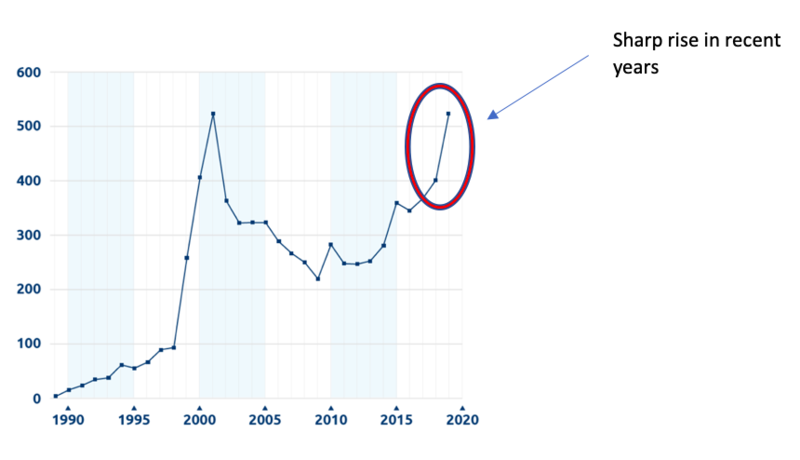
Below is a graphic demonstrating the numbers LDLTs over time. As detailed, only in the last few years have the numbers of LDLTs performed increased substantially.
We will now review the reasons why we use LDLT in children and then in adults.
Why do we use LDLT in pediatrics?
LDLT is more commonly used in pediatrics than in adults and has become more widely used in pediatrics in the past decade. In fact, according to 2018 SRTR data, about 11% of pediatric liver transplants in the US were from living donors! LDLT is a consideration in any pediatric liver transplant candidate, though it is a particularly desirable choice for children with longer waitlist times and for younger children. Children under the age of 1 have the highest risk of pretransplant mortality, and the acuity of pediatric patients on the waitlist is rising presumably due to lack of access to suitable donor organs.
Finding an appropriately sized whole organ or split graft in the deceased donor organ pool can be challenging for pediatric patients, and particularly for infants and toddlers on the waitlist. Given that over half of all children listed for liver transplant are 5 years or younger, this is a major issue. Notably, under the current allocation system, roughly half of all pediatric donor livers were allocated to adult recipients. Additionally, we can see large for size syndrome in pediatric liver transplantation. The size discrepancy between vascular structures can lead to insufficient blood supply to the graft, abdominal compartment syndrome, and other complications.1 Prior to LDLT, centers would often cut grafts to fit pediatric patients, thereby discarding the unused segment, or perform split grafts whereby deceased grafts were divided into two segments to be used in two different recipients. The latter was surgically complex and logistically complicated, thereby limiting its use, but the techniques learned paved the way for the eventual development of LDLT. For all these reasons, LDLT, when feasible, provides an attractive option for pediatric patients awaiting liver transplantation.
One unique application of LDLT in a specific pediatric population is for the treatment of metabolic liver diseases, including Wilson’s disease, alpha-1-antitrypsin deficiency, organic acidemias, and urea cycle disorders apart from OTC deficiency. Though liver transplantation provides definitive treatment for many of these conditions, some patients can wait a long time for an appropriate decreased donor graft which puts them at risk for complications including metabolic crises and permanent neurologic damage depending on their underlying disease. LDLT offers a way to treat these disorders. Currently <10% of pediatric LDLT cases are used for this purpose, despite metabolic liver diseases making up ~16% of all pediatric liver transplants. The hesitancy to use LDLT in metabolic disease is often attributed to fear of limited efficacy from heterozygous donors; however, use of heterozygous donors has been demonstrated to be safe and has led to the correction of metabolic disorders for most recipients.
Is there an immunologic benefit for children who receive liver transplants from their parents?
Possibly! Research in this area supports that children who receive grafts from their mothers may be at an advantage. A recent review analyzed data from multiple centers in the US, Japan, and Europe and found that pediatric LDLT recipients, particularly patients with biliary atresia who have received grafts from their mothers, have lower rates of acute cellular rejection and post-transplant graft failure. Proposed mechanisms of this immunologic benefit were maternal-fetal micro chimerism and persistence of T-regulatory cells. Pediatric LDLT recipients of maternal grafts may be able to achieve operational tolerance (clinical state of allograft acceptance), thereby permitting the withdrawal of immunosuppression.
Why do we use LDLT in adults?
Compared to pediatric LDLT, LDLT in adults makes up a smaller portion of all transplants performed each year. Over the past two decades, <5% of all LTs have been LDLTs. Though LDLT could address the growing organ shortage across all indications for LT in adults, there are specific situations in which it is particularly useful:
1) Patients with low MELD scores.
LDLT has a very important benefit over DDLT in that a patient does not have to wait until he/she is very sick (high MELD) to get an organ. This is particularly important in patients with low MELD scores but other debilitating symptoms of cirrhosis including refractory ascites or variceal bleeding. Of course, for patients with very low MELD scores and few complications of cirrhosis, the risk of surgery to both recipient and donor must be weighed against the benefits.
2) Patients with hepatocellular carcinoma (HCC).
Despite exception points, which expedite the path to transplant for patients with HCC, there are many who still need to wait a significant amount of time on the waiting list prior to transplant. During this time, tumors may grow outside of Milan criteria, thereby making the patient non-transplantable (see more about exception points and Milan’s criteria in my previous post). Though much has changed since the UNOS new organ allocation policies, the progression of HCC while on the waiting list is still estimated to be high. In a recent study analyzing the period between 1995 and 2014, overall survival from the time of listing was higher for LDLT than for DDLT, though in propensity score analysis, there was no difference in recurrence-free and overall survival.
LDLT additionally offers the option to transplant those with HCC outside of Milan criteria. Studies from Asia have suggested that expansion of criteria to include larger size and greater number of tumors has led to comparable outcomes compared to Milan criteria tumors.
3) Patients with cholestatic liver disease and recurrent cholangitis
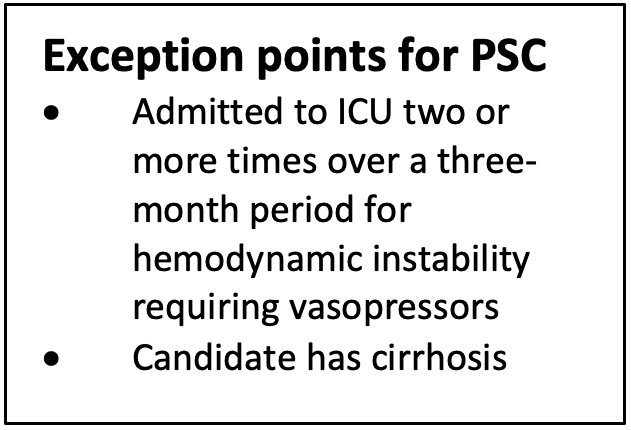
Though primary sclerosing cholangitis (PSC) is a condition that gives patients exception points for transplantation, the criteria required for these exception points is fairly strict. Many patients have recurrent cholangitis requiring long courses of IV antibiotics, but because of early recognition, do not necessarily become sick enough to require ICU admission. LDLT offers an additional route to transplantation of this specific population.
What are the outcomes for pediatric and adult LDLT?
Overall, outcomes after LDLT in both adult and pediatric patients are quite good!
In a recent review of SRTR data for pediatric transplants from 2002-2017, it was reported that overall the outcomes for technical variant grafts have been improving, and that outcomes for LDLT may superior to DDLT. In this study, one-year patient survival was 96% for LDLT and graft survival at one year was 91% during the entire studied period, and 94% from 2010-2015. Additionally, compared to whole liver transplants, LDLT had a lower risk of graft failure at one year with an adjusted hazards ratio of 0.71.
For adults, the Adult-to-Adult Living Donor Liver Transplantation Cohort Study (A2ALL), a multi-center study investigating recipient and donor outcomes in LDLT, has led the way in LDLT research in the US. The original study demonstrated that 90-day and 1-year survival was >80%, and after following patients prospectively, 10-year survival was actually higher than for DDLT.
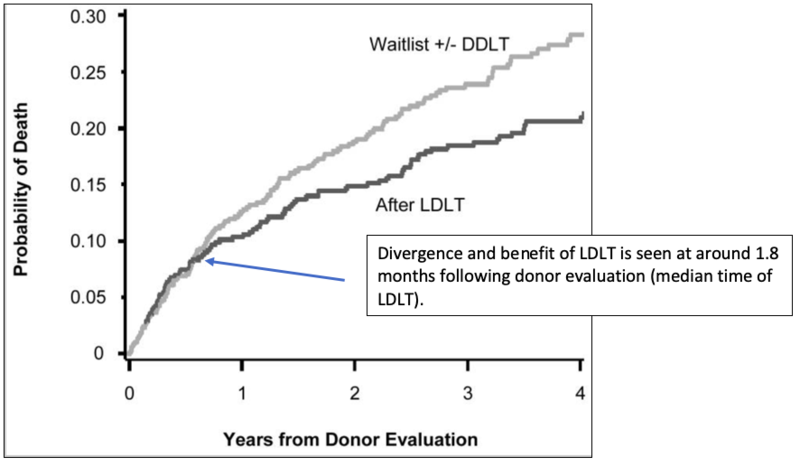
Many of the prior analyses of LDLT outcomes focused on outcomes after transplantation but did not consider mortality while awaiting transplantation. Much of the 10-year survival benefit in this latter study was secondary to reduced waitlist mortality given patients receiving LDLT were transplanted at a lower MELD score and did not have to wait as long on the waiting list. A recently published meta-analysis also found that LDLT was associated with reduced mortality of >10% at 5-years compared to DDLT with similar graft survival and lower risk of rejection. Much of this benefit was also attributed to preoperative variables, such as lower MELD at transplant and shorter waiting times.
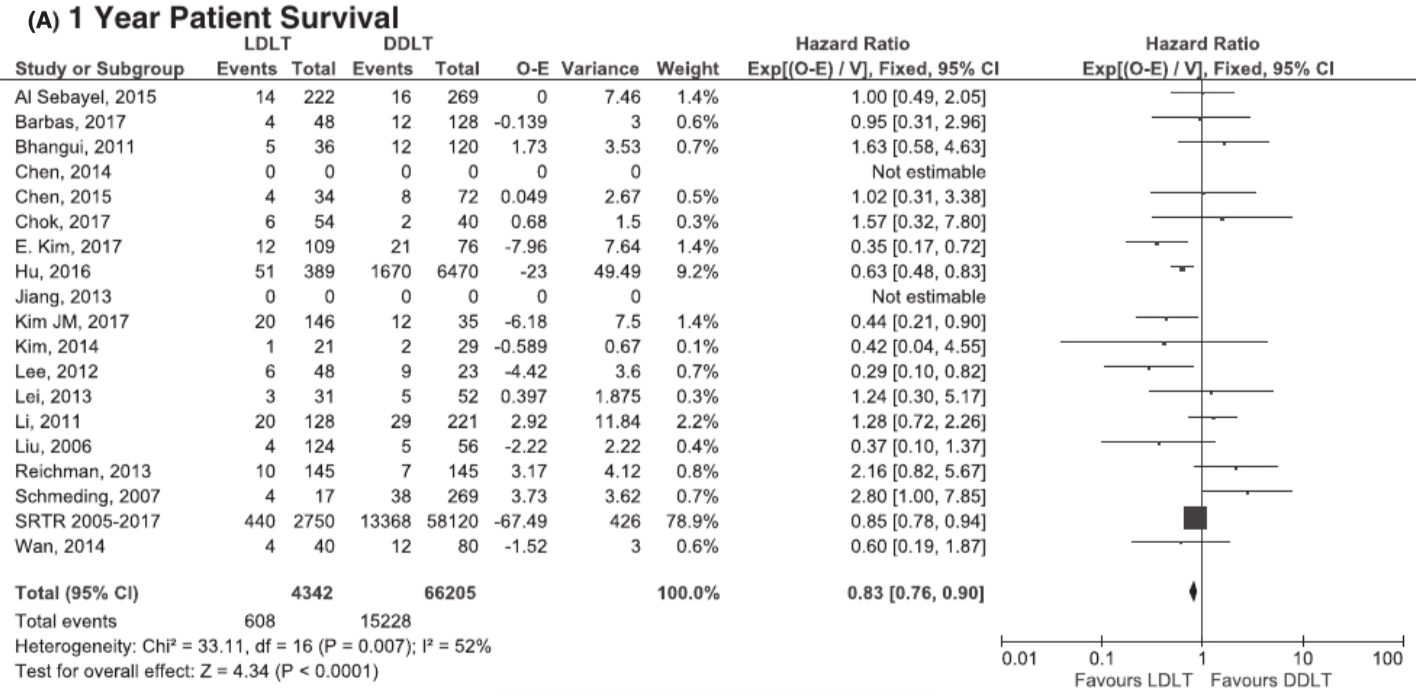
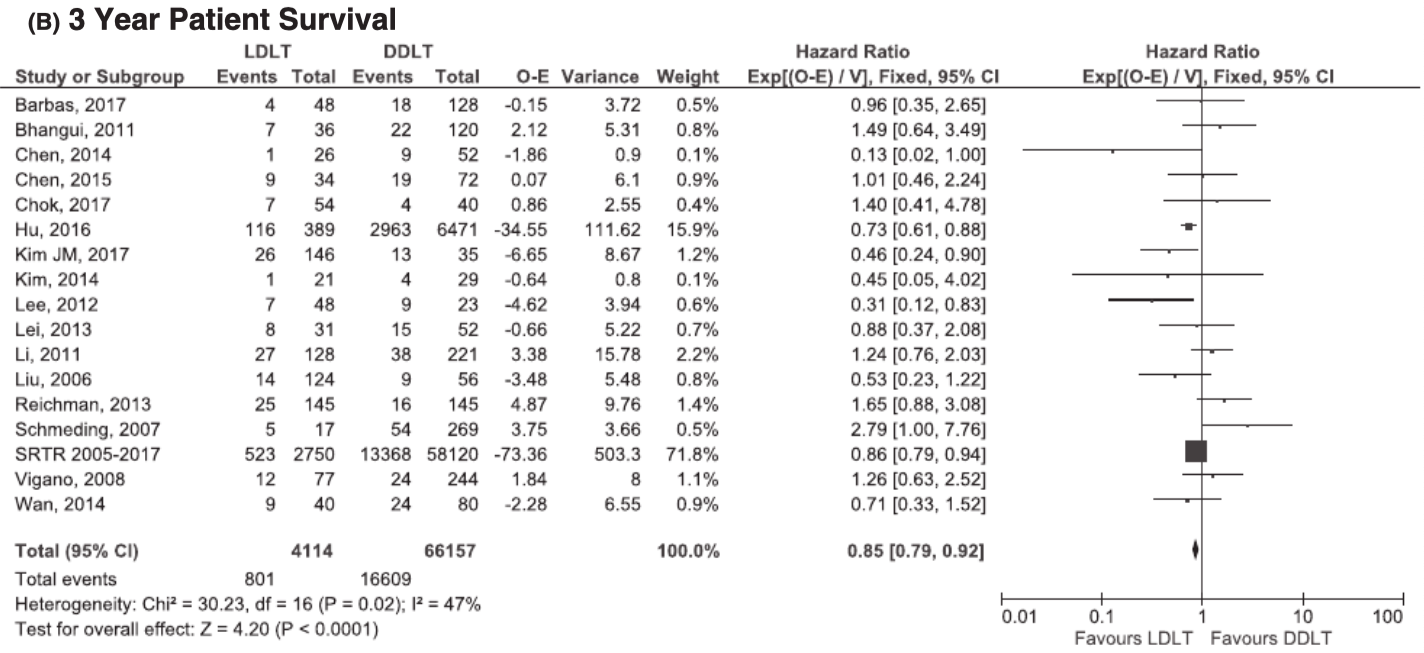
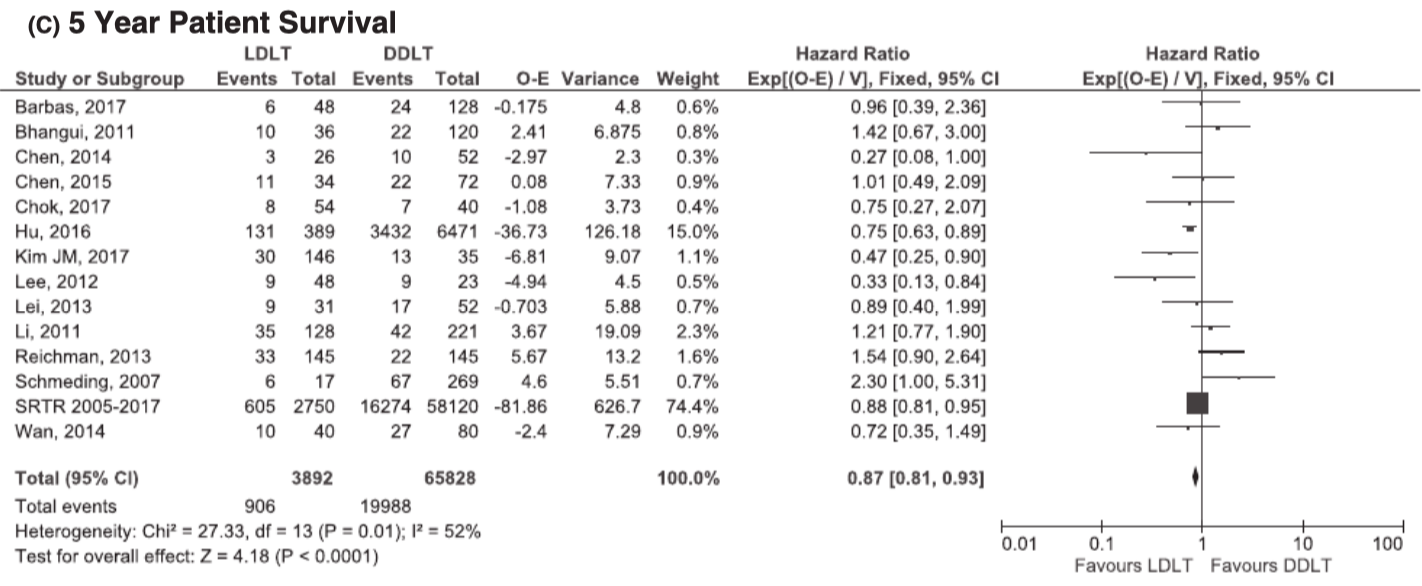
In the above three graphs, 1-, 3-, and 5-year survival all demonstrate a survival benefit with LDLT.
A third study looking at patients with MELD>25 and hepatorenal syndrome (a group that traditionally felt to be “too sick” for LDLT) found that compared to DDLT, those with LDLT had improved 5-year overall survival, again attributed to decreased waitlist mortality.
In addition to decreased time on the waiting list and transplantation at lower MELD, LDLT also has the benefit in that it is an elective surgery where anatomic variants can be planned out and programs can screen an ideal donor. As additional centers begin to perform LDLT and as LDLT is used for non-traditional indications, we will have to continue to study outcomes, focusing not only on post-transplant survival, but also on pre-transplant factors, such as reduced waitlist mortality.
What are the complications for pediatric and adult LDLT?
Biliary complications have been described as the “Achilles heel” of LDLT, and this is true in both pediatric and adult cases. In recent review of pediatric LDLT, the study group identified in multivariate analysis that hepaticojejunostomy without external stent placement was an independent risk factor for anastomotic stricture formation. Roux en Y hepaticojejunostomy, which could lead to anastomotic strictures, is necessary in patients undergoing transplant for biliary atresia (the most common indication for pediatric liver transplantation), and for smaller patients where a duct-to-duct anastomosis is not feasible given recipient duct size. For adult patients, though biliary complications may be more common in LDLT than DDLT, treatments and time to resolution seem to be similar for the two types of transplant.
What about complications for the donors?
Living donors to both pediatric and adult recipients are subject to similar complication rates, though donors to pediatric recipients are often able to donate a left lobe or left lateral segment (which leads to fewer complications), while donors to adult recipients more often must donate a right lobe. For living donors, the most common complications include bacterial infections, biliary complications, with many fewer experiencing intraoperative complications, incisional hernias, and pleural effusions. Though most donors report a good quality of life after donation and many would donate again, some developed psychological distress and a majority experienced socioeconomic concerns.
What are the potential barriers to LDLT?
Many socioeconomic factors impact the decision to pursue LDLT, and these factors likely do not differ significantly between pediatric and adult LDLT. Most donors and recipients of LDLT are white and have private insurance compared to in deceased whole liver or split liver transplants. The out-of-pocket cost for LDLT can actually be prohibitive for many patients. Short-term and hospital related costs are often covered by the recipient’s insurance, but late complications and future hospitalizations may not be covered. Additionally, travel and lodging are often not reimbursed. One study estimated that the mean out-of-pocket costs for donors is almost $4,000.
Lack of education and awareness of LDLT is another important factor to consider. In a recent survey study of families with children who had a recent liver transplant or were on the transplant waitlist, 97% of respondents understood that LDLT was possible, 72% knew the steps in evaluation and only 69% knew that the donor surgery was covered by the recipient’s insurance. In this study, individuals with public insurance were less likely than those with private insurance to know about steps of evaluation for LDLT and were significantly less likely to feel well-informed and to understand how donor surgery may impact time off from work.
Given the potential benefits of LDLT as well as the safety for donors and recipients, it will be imperative in the future to work to address these and other barriers. By increasing the numbers of LDLTs performed, we can hopefully begin to address the growing organ shortage in the United States.