Hepatitis C You Later!

Hepatitis C Virus and Direct-Acting Antivirals: The Basics
Hepatitis C virus is an RNA virus with a narrow species and tissue tropism: it replicates effectively only in humans and in chimpanzees and only in liver tissue. To date, 6 genotypes have been identified: 1a, 1b, and 2 through 6. The entire HCV RNA strand is contained on a single open reading frame which encodes a polyprotein of around 3000 amino acids. This includes structural proteins, the viral core and envelope proteins, and “non-structural” proteins (NS2, NS3, NS4B, NS5A, NS5B), which include the viral polymerase, protease, and assembly and release proteins. The sequencing of the HCV genome and detailed discovery of the HCV life cycle paved the way for the development of the new generation of anti-viral therapies called direct-acting antivirals, or DAAs. In fact, non-structural proteins are the targets for DAAs, which interfere directly and specifically with these viral proteins required for replication.
The first DAAs were in the class of protease inhibitors (PIs), which inhibit the splicing of the HCV polyprotein by the HCV NS3 or NS4A protease. Protease inhibitors have been used to treat other viruses, such as human immunodeficiency virus (HIV). The major milestone towards HCV cure was the development of NS5A inhibitors as an entirely new drug class, which, in contrast to protease inhibitors, has not been used for any other viral infection. Today, NS5A inhibitors are part of every DAA regimen.
Who Should be Treated?
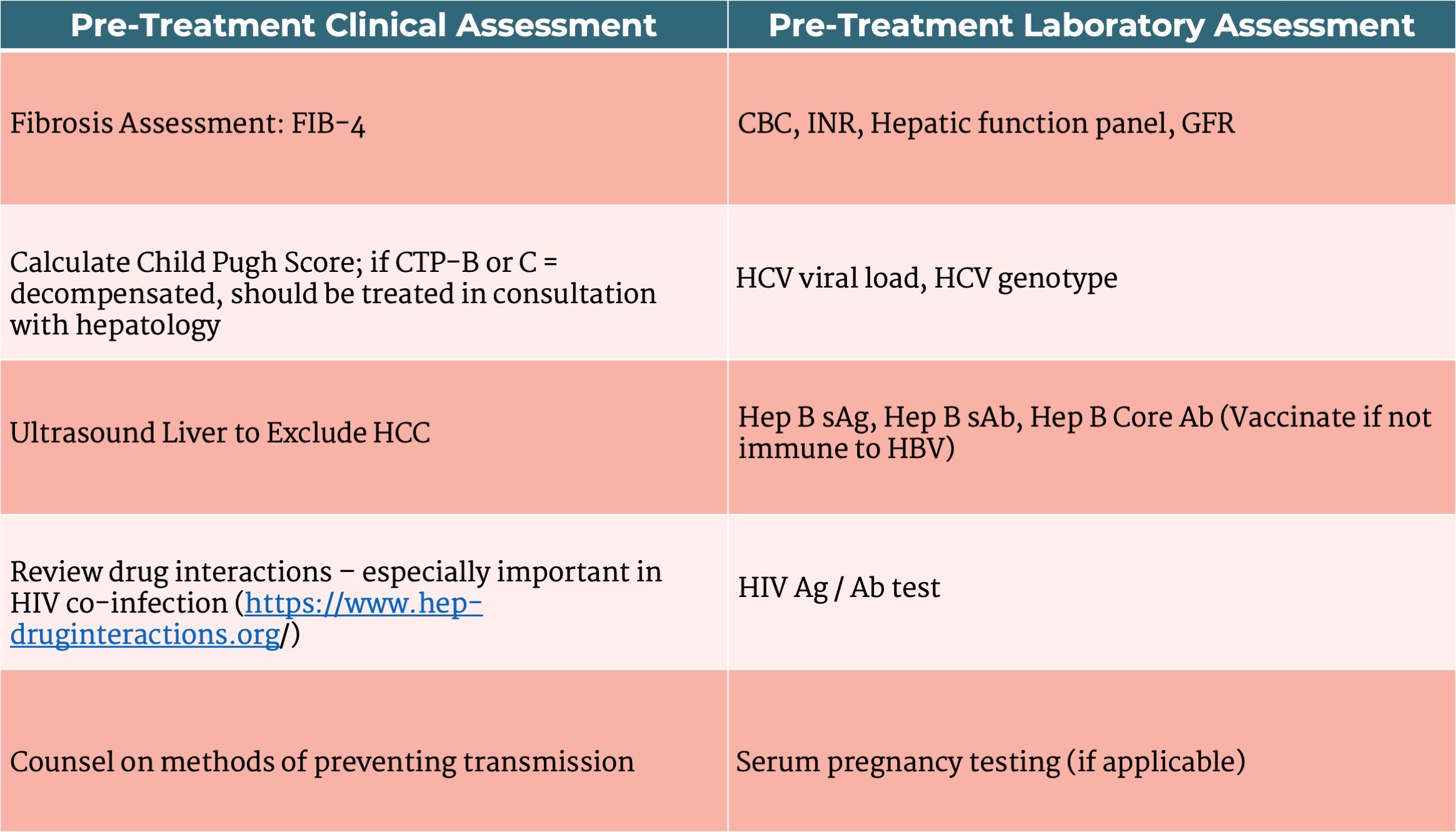
Pre-Treatment Assessment
Evaluation for co-infection with hepatitis B virus (HBV) and human immunodeficiency virus (HIV) is recommended because these conditions may accelerate fibrosis and are associated with poorer prognosis. Specifically, for patients with chronic hepatitis B infection (Hep B sAg positivity), there is a risk of reactivation of hepatitis B infection with HCV treatment, and according to AASLD guidelines, these patients should receive additional monitoring during treatment. Patients who otherwise meet criteria for HBV antiviral therapy should be started on this. It is common practice to initiate patients on HBV antiviral therapy prior to initiation of HCV treatment and continue HBV therapy for 12 weeks after completion to prevent HBV vaccination. However, this is not specifically recommended in AASLD guidelines, and close monitoring of liver enzymes and HBV DNA viral load is still considered an acceptable alternative. Patients with hepatitis B core Ab positivity (with or without sAb positivity) and sAg negativity have a cleared HBV infection and do not require additional monitoring or therapy in the context of HCV treatment.
Table 1. Pre-treatment Assessment
Recommended Treatment Regimens
DAA therapy has revolutionized the treatment of HCV, leading to viral eradication in the vast majority of patients who are treated. The treatments are simple to administer - all oral, once daily tablets, usually lasting for 12-24 weeks – and are generally well-tolerated, with no or only minor adverse effects.
Ledipasvir/sofosbuvir, or Harvoni®, was the first fixed-dose combination DAA that substantially simplified HCV therapy. It was initially studied for 12-24 weeks of treatment, and subsequently, the 8-week course was shown to be non-inferior to the 12 week regimen. However, ledipasvir has relatively low efficacy against genotypes 2 and 3. As a result, its use was restricted to genotypes 1, 4, 5, and 6. This medication is considered safe in patients with decompensated cirrhosis.
The next wave of DAAs brought the advantage of pan-genotypic regimens. Pan-genotypic therapies are highly effective against HCV genotypes 1 through 6, are simple to implement, and, in theory, eliminate the need to check an HCV genotype. This approach is sufficient for the majority of patients, and the simplicity of this approach is essential when aiming for HCV elimination on a global scale.
Glecaprevir/pibrentasvir, or Mavyret®, is a second pan-genotypic regimen. It is available in a two-drug fixed-dose combination containing 100 mg of glecaprevir and 40 mg of pibrentasvir. The recommended dose is 3 tablets taken orally once daily with food, as glecaprevir’s absorption is improved with food, for 8 weeks. When compared to patients with normal hepatic function, the concentration of glecaprevir was significantly higher in patients with moderate or severe (Child Pugh B or C) hepatic dysfunction. Because of this, glecaprevir/pibrentasvir should not be used in patients with Child-Pugh B or C cirrhosis. It is safe for use in advanced CKD and ESRD on dialysis. The most commonly reported side effects of Mavyret® were headaches and fatigue.
Sofosbuvir/velpatasvir, or Epclusa®, can be used for Genotypes 1, 2, and 4-6; patients with genotype 3 require baseline NS5A resistance-associated substitution testing. Those without Y93H can be treated with Epclusa®. Those with Y93H should be treated with glecaprevir/pibrentasvir or (if unavailable), can be treated with sofosbuvir/velpatasvir + weight-based ribavirin OR an alternative DAA, sofosbuvir (400 mg)/velpatasvir (100 mg)/voxilaprevir (100 mg), Vosevi®. Sofosbuvir/velpatasvir is available in a two-drug fixed-dose combination containing 400 mg of sofosbuvir and 100 mg of velpatasvir in a single tablet for 12 weeks. The recommended dose of the combination is 1 tablet taken orally once daily with or without food. This is safe for use in patients with decompensated cirrhosis and in patients with advanced CKD / ESRD on HD. In patients with decompensated cirrhosis and HCV genotypes 2 and 3, this is the preferred option since ledispavir/sofosbuvir does not cover genotypes 2 and 3. Headache, fatigue and nausea are the most commonly reported adverse events, at a similar frequency to placebo-treated patients. Of note, sofosbuvir can cause significant bradycardia when taken with amiodarone so this is a contraindication to sofosbuvir-based DAA regimens. Certain anti-epileptics are also contraindicated, and interactions can be checked at: https://www.hep-druginteractions.org/.
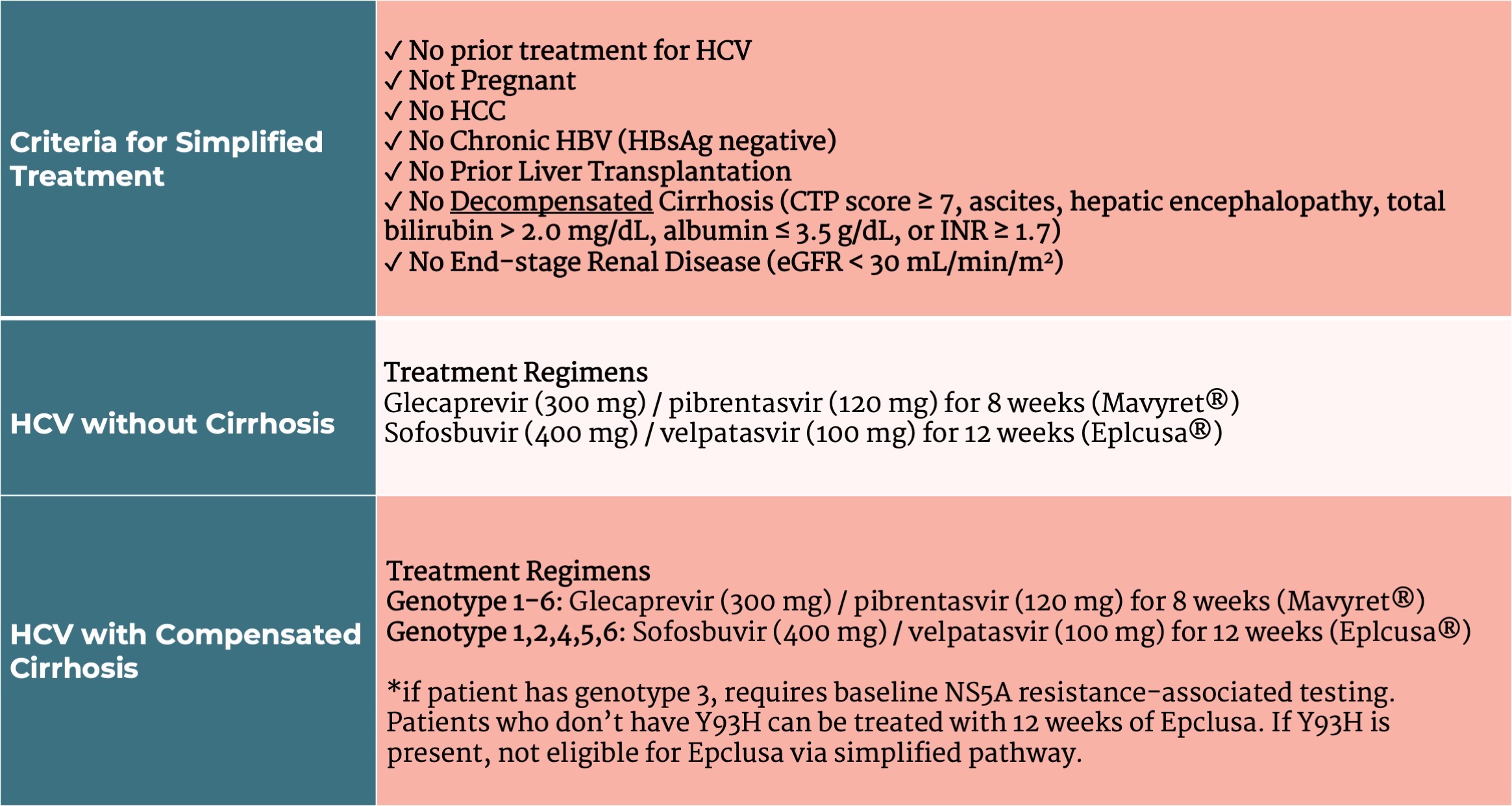
Both glecapravir/pibrentasvir and sofosbuvir/velpatasvir are highly effective in treatment-naïve adults with compensated cirrhosis, regardless of HCV genotype. Because of this, AASLD and EASL propose the use of either of these 2 pan-genotypic regimens in patients without cirrhosis or patients with well-compensated cirrhosis who are treatment naïve. (Table 2)
Table 2. Simplified Treatment of Hepatitis C
Post-Treatment Monitoring:
Treatment of HCV reduces all-cause mortality and also liver-related adverse consequences including cirrhosis and HCC. The goal of treatment is sustained virologic response, or SVR. SVR means that the hepatitis C virus is not detected in the blood 12 weeks or more after completing treatment. SVR is a marker of cure of HCV infection and has been shown to be durable in large prospective studies in more than 99% of patients with 5+ years of follow-up. Documentation of SVR requires an FDA approved quantitative or qualitative nucleic acid test with detection level of < 25 IU / mL. For post-treatment assessment, after confirming SVR, if non-cirrhotic – no liver-related follow up is recommended. If a patient has cirrhosis or advanced fibrosis, they will need continued HCC screening and evaluation and management of portal-hypertensive complications.
Re-treatment:
Although cure rates are extremely high (>95%), a small portion of patients will fail to respond to first line DAA therapy. For these patients, EASL recommends sofosbuvir/valepatasvir/voxilaprevir, or Vosevi®.
Contraindications and Additional Considerations:
Currently, hepatitis C treatment is contraindicated in patients who are pregnant or breastfeeding due to a lack of studies demonstrating their safety. Treatment of patients with decompensated cirrhosis, HIV and/or HBV co-infection, prior liver transplantation, HCC, ESRD may require additional considerations. Patients with a short life expectancy due to advanced liver disease are recommended to be managed in consultation with a liver specialist.
In Summary:
Direct-acting antivirals have revolutionized treatment of HCV. The extremely high cure rates associated with DAAs have changed the way we think about HCV and HCV treatment and have even changed the landscape of liver transplantation. They have allowed us to expand the donor pool to include HCV-positive donors for HCV-negative recipients, and treat recipients post-transplantation with extremely high rates of cure.