Acute Viral Hepatitis: Non-Hepatotropic Viruses

Brief Case Presentation
This patient underwent haplocord stem cell transplantation in the setting of acute myeloid leukemia (AML) approximately 2 months prior to presentation. Post-transplant course was complicated by acute graft-versus-host disease (GVHD), necessitating hospital admission and an extended course of steroids. The patient received standard prophylaxis for common opportunistic infections throughout this time. While completing a steroid taper as an outpatient, the patient developed abdominal cramping and profuse watery diarrhea, prompting re-admission and empiric initiation of intravenous steroids.
GI infectious panel and CMV PCR upon admission were negative, but a subsequent adenovirus PCR was positive. Colonoscopy performed on day 2 of admission revealed adherent blood, congestion, erythema, friability, and shallow ulcerations throughout the entire colon. EGD showed mild erythema in the pre-pylorus but was otherwise unremarkable. Biopsies of the colon were consistent with acute GVHD with superimposed adenovirus inclusions. The antrum and duodenum were likewise involved by acute GVHD, though no viral inclusions were identified. Given the diagnosis of adenovirus colitis and viremia, cidofovir was initiated.
Of note, the patient’s liver chemistries were predominantly normal upon admission, but progressively up-trended, as summarized in Table 1. The differential included drug-induced liver injury (DILI) versus adenovirus hepatitis.
Table 1. Liver function tests during admission
| Day of admission (day 0) | Liver function test values at time of liver biopsy (day 14) | |
| AST [normal, 8-37 U/L] | 27 U/L | 409 U/L |
| ALT [normal, 8-35 U/L] | 28 U/L | 463 U/L |
| Alkaline phosphatase [normal, 30-120 U/L] | 222 U/L | 660 U/L |
| Total bilirubin [normal, 0.1-1.0 mg/dL] | 0.4 mg/dL | 5.8 mg/dL |
| Conjugated bilirubin [normal, 0.0-0.3 mg/dL] | 0.1 mg/dL | 5.7 mg/dL |
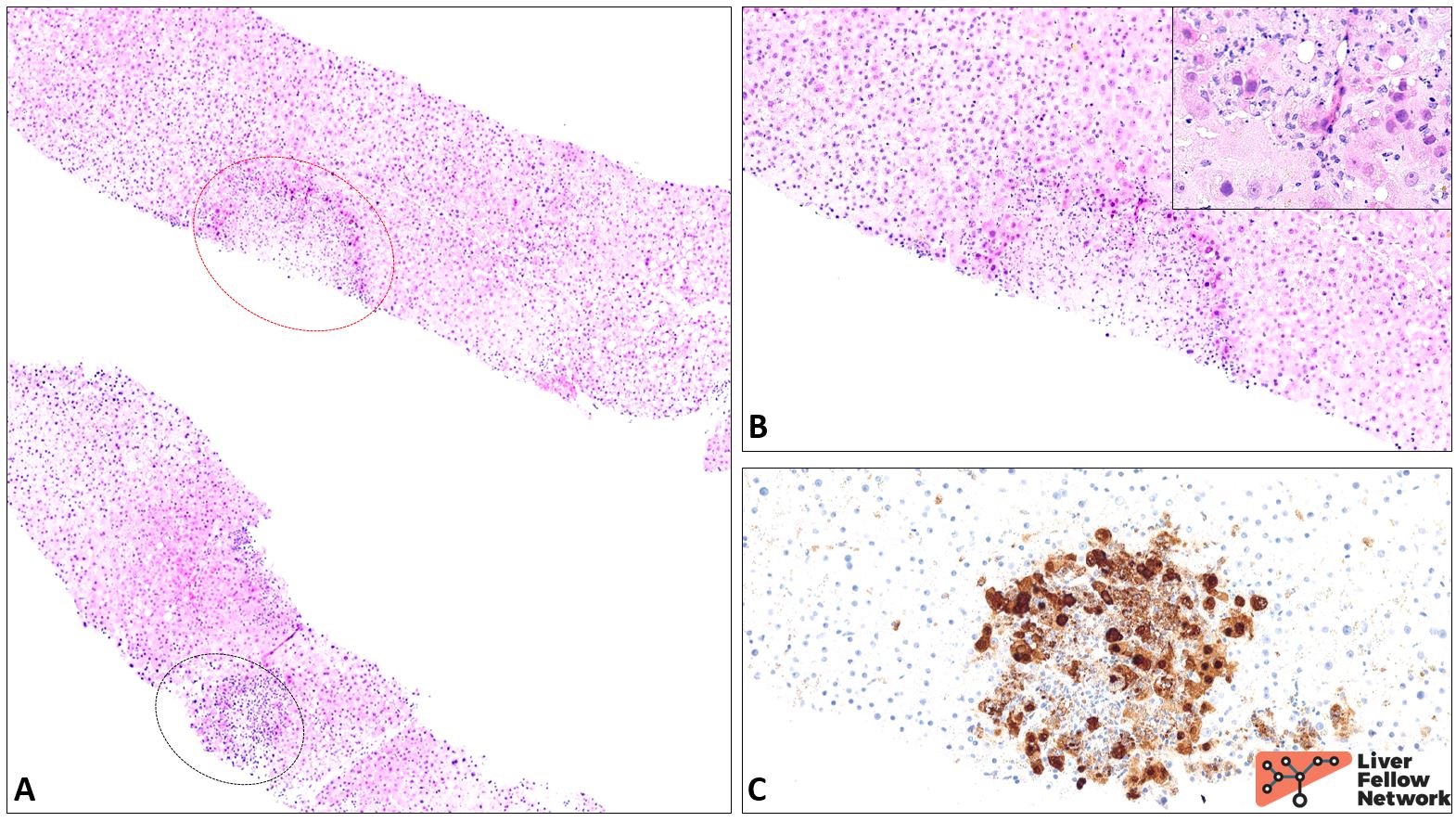
Figure 1. Liver biopsy on day 14 of admission. As seen at low power in A, the most striking feature of this biopsy is the presence of multifocal necrosis within the lobular parenchyma. The necrotic regions are relatively well-demarcated, and the viable hepatocytes along the rim exhibit abnormal nuclei with “smudgy” chromatin (B, with inset; corresponds to red-circled area in A). This finding is classic for adenovirus, as confirmed by an immunostain (C; corresponds to black-circled area in A). The remainder of the biopsy is essentially unremarkable: the portal tracts exhibit a mild lymphocytic infiltrate, but there is no bile duct damage. There is no steatosis, cholestasis, or necro-inflammatory activity within the lobular parenchyma. There is no evidence of GVHD, veno-occlusive disease/sinusoidal obstruction syndrome, or involvement by recurrent AML.
Non-Hepatotropic Viral Hepatitis: An Overview
Though the term “viral hepatitis” typically brings to mind acute/chronic infection with hepatitis A through E, an array of non-hepatotropic viruses can also cause acute hepatitis, albeit rarely. These include cytomegalovirus (CMV), Epstein-Barr virus (EBV), adenovirus (as discussed in the opening vignette), and herpes simplex virus (HSV)-1 and -2. The clinical presentation ranges from self-limited mild transaminitis and malaise to fulminant hepatitis; not surprisingly, infections are most common and generally most severe in immunocompromised patients. In this population in particular, hepatitis may represent just one facet of systemic/disseminated disease (e.g., disseminated adenovirus infection, as seen above), though liver-limited infections may also occur. The post-transplant setting presents additional clinical and diagnostic complexities, as infection and acute cellular rejectionmay overlap clinically and accurate histologic diagnosis is key to appropriate management.
These cases exhibit a spectrum of histologic findings: while outright necrosis and unequivocal viral inclusions, when present, make for a fairly straightforward diagnosis, the histologic features may conversely be fairly subtle and nonspecific, and pathognomonic inclusions are not always readily identified. Pathologist awareness of these entities and close clinical correlation are therefore crucial. Below, we briefly review the classic histologic findings seen in several of the more common non-hepatotropic viral hepatitides.
Cytomegalovirus (CMV)
CMV, a double-stranded DNA virus from the Herpesviridae family, is one of the most common causes of opportunistic viral hepatitis in liver transplant recipients. Patients typically present within the first 3 months post-transplant. Donor/Recipient serologic profile is an important risk factor: seronegative patients receiving allografts from seropositive donors are at highest risk of post-transplant CMV hepatitis (up to approximately half to two-thirds of patients without prophylaxis), though seropositive recipients may also experience viral reactivation in the setting of transplant-related immunosuppression. In the immunocompetent population, CMV infection is generally subclinical, but may present with symptoms resembling infectious mononucleosis (malaise, fatigue) and a mild hepatitis.
In the liver, CMV exhibits tropism for endothelial cells as well as hepatocytes, biliary epithelial cells, and macrophages. Infected cells show characteristic cytoplasmic enlargement (“cytomegaly”) and nuclear and cytoplasmic viral inclusions, which may be either deeply eosinophilic or basophilic. The inclusions are classically surrounded by a pale rim, giving the appearance of “owl eyes.” Unfortunately, these viral cytopathic changes may not always be present, particularly on small biopsies, and their absence does not rule out a diagnosis of CMV hepatitis. Immunohistochemistry (IHC) or, less commonly, in situ hybridization (ISH) may help to clarify the diagnosis if definite inclusions are not identified on H&E.
Though nonspecific, clusters of neutrophils (“microabscesses” or “mini-microabscesses”), classically centered around an infected hepatocyte, are another helpful clue. Their presence in an immunocompromised patient, even in the absence of viral inclusions, should prompt consideration of CMV infection. Mild portal and lobular lymphocytic infiltrates are also common findings, though crucially, lymphocytic cholangitis and endotheliitis – hallmarks of rejection when seen in an allograft – are absent. Sinusoidal lymphocytosis in a linear (“string of beads”) configuration may be present, particularly in immunocompetent patients. Occasional hepatocyte ballooning may also be observed.
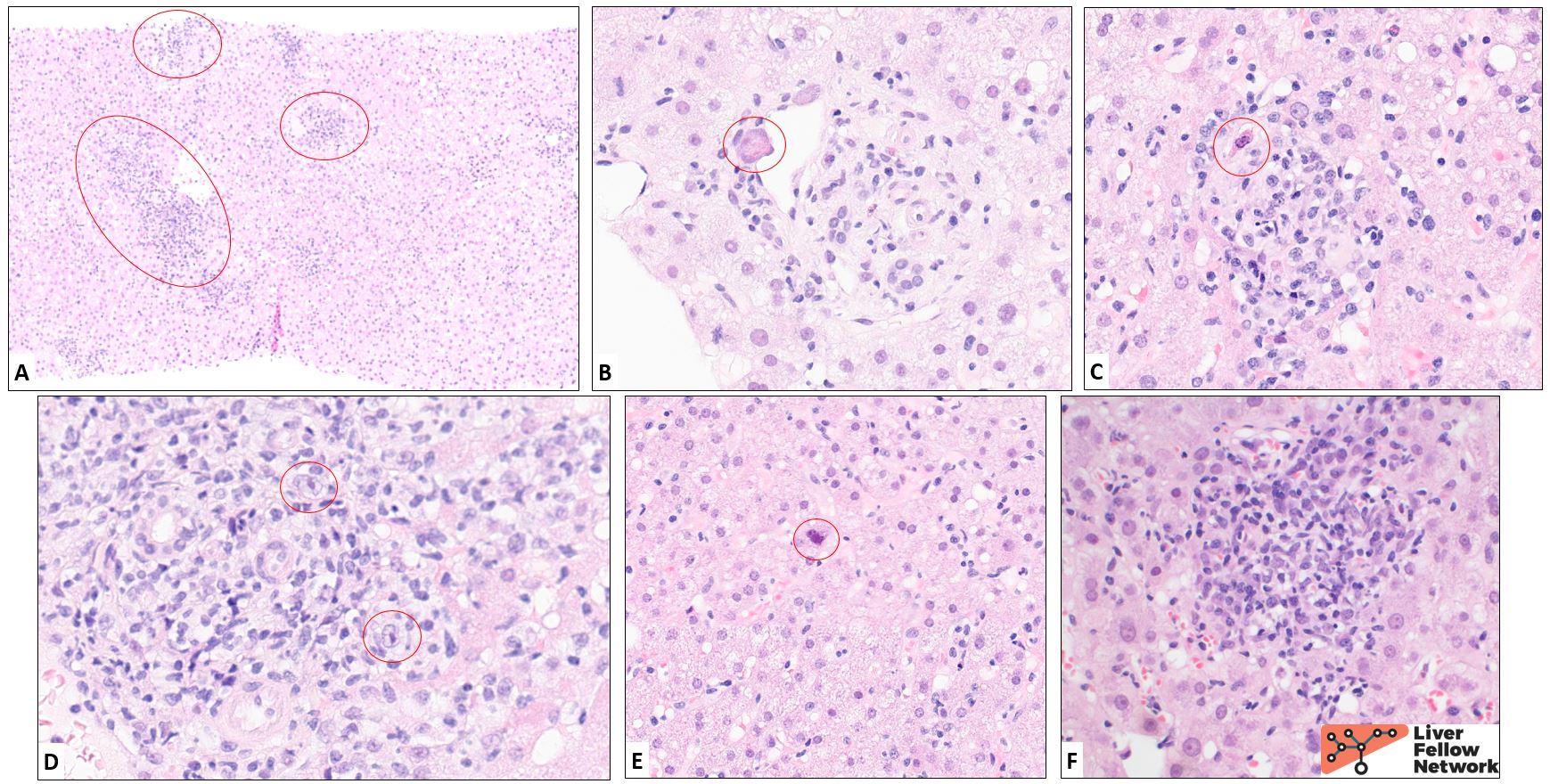
Figure 2. Biopsy from a patient with a history of cirrhosis in the setting of hepatitis C infection, now status post antiviral therapy with sustained virologic response, followed by orthotopic liver transplantation. Approximately 7 months post-transplant, the patient developed low-grade fevers and diarrhea. Liver function tests were as follows: AST 125 U/L, ALT 143 U/L, alkaline phosphatase 283 U/L, and total bilirubin 0.5 mg/dL. A biopsy was performed with a working differential of acute cellular rejection versus DILI. At low power (A), the biopsy demonstrates patchy portal and lobular inflammation (circled in red). Inspection at higher power reveals characteristic CMV inclusions (circled in red) in portal vein radicle endothelial cells (B), portal tract stromal cells (C, D), and hepatocytes (E). Ganciclovir therapy was initiated with clinical improvement, as reflected on a biopsy taken approximately 2 weeks later, which showed small scattered microabscesses (F) but no viral inclusions (confirmed by negative immunostain). Of note, features suspicious for acute cellular rejection (not shown here) were also present in both biopsies; this may have further contributed to the patient’s liver dysfunction. Images B and F courtesy of Dr. Lindsay Alpert, Department of Pathology, University of Chicago Medicine.
Epstein-Barr Virus (EBV)
Hepatic involvement by EBV typically occurs as an opportunistic infection in immunocompromised patients, or in the setting of infectious mononucleosis in immunocompetent individuals (typically young adults); isolated EBV hepatitis in otherwise healthy patients can also occur, though rarely. Like CMV, EBV is a double-stranded DNA virus and a member of the Herpesviridae family. However, viral tropism in the liver is generally limited to lymphocytes (predominantly B-cells, with a minor T-cell component), though very rare exceptions do occur (e.g., EBV-associated spindle cell tumors). The infected lymphocytes may exhibit mild reactive atypia but no inclusions. Biopsies demonstrate a predominantly lobular lymphocytic infiltrate; sinusoidal lymphocytosis with a characteristic “string of beads” arrangement is a classic, though non-specific, feature. Hepatocyte injury is quite mild irrespective of the degree of inflammation, with only rare acidophil bodies or occasional small non-necrotizing epithelioid granulomas appreciated within the lobules. A modest portal lymphocytic infiltrate, sometimes showing mild atypia, is also common; spillover into the surrounding parenchyma may be seen, but there should be no outright interface activity. Ancillary testing, through either EBV encoding region RNA (EBER) ISH or alternatively, EBV-latent membrane protein (LMP-1), is necessary to confirm the diagnosis.
The histologic differential includes chronic hepatitis C infection, drug-induced liver injury, and hepatic involvement by leukemia/lymphoma, e.g., chronic lymphocytic leukemia. CMV hepatitis in immunocompetent patients may also demonstrate sinusoidal lymphocytosis. Of note, post-transplant lymphoproliferative disorder (PTLD) is also an EBV-driven process, but would present with a destructive mass-forming lesion rather than a diffuse lobular infiltrate.
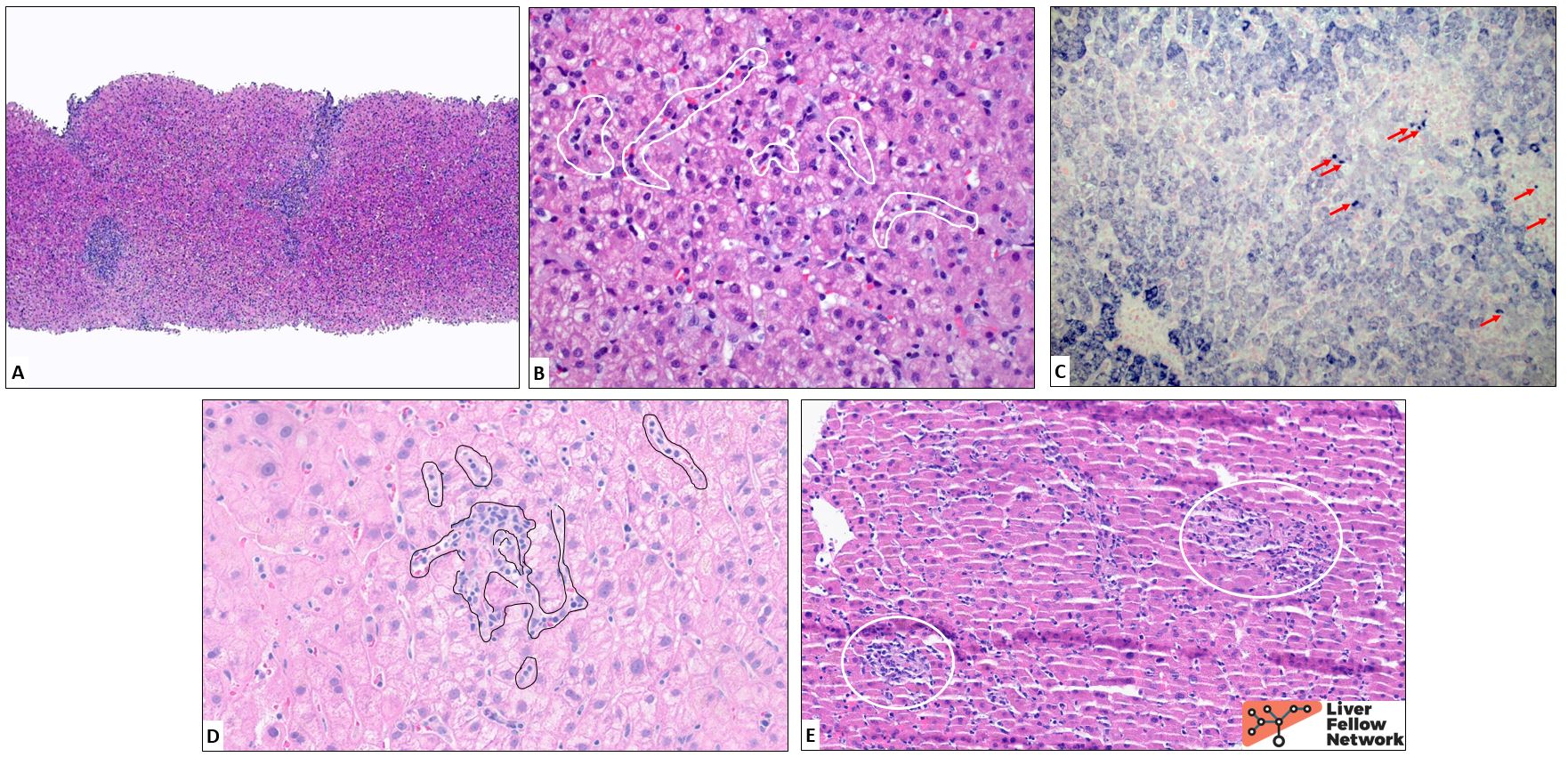
Figure 3. This liver biopsy from a patient presenting with fatigue, malaise, hepatosplenomegaly, and mild transaminitis demonstrates a dense, predominantly lymphocytic portal infiltrate (A) as well as a mild sinusoidal lymphocytic infiltrate (B, marked in white). EBER ISH shows scattered strongly positive lymphocytes within the sinusoidal infiltrate (C, red arrows). Classically, the lymphocytic infiltrate exhibits a “string of beads” arrangement within sinusoids (marked in black in D;image from a different case). Small non-necrotizing epithelioid granulomas (E, circled in white; image from a different case) are also a helpful, though nonspecific, feature. Images A-C courtesy of Dr. John Hart, Department of Pathology, University of Chicago Medicine.
Adenovirus
Adenovirus is a double-stranded DNA virus that most commonly causes respiratory tract infections and/or conjunctivitis in immunocompetent children, but can also cause acute hepatitis in the setting of immunosuppression. Liver transplant recipients are at highest risk, followed by bone marrow transplant recipients; infection typically occurs within the first 6 months post-transplant and children are particularly susceptible. Infections are often devastating, with mortality rates of nearly 75%. As seen in the opening vignette, biopsies demonstrate variable necrosis in a non-zonal distribution, ranging from small, relatively well-demarcated areas to wide swathes involving much of the core. The nuclei of the hepatocytes at the rim of the necrotic areas generally contain basophilic nuclear inclusions that impart a “smudgy” look to the chromatin. Anti-adenovirus IHC can help to confirm the presence of viral particles and rule out reactive atypia, which may pose a diagnostic challenge in these cases. The remaining viable parenchyma often shows a scattered lymphocytic infiltrate, typically quite mild relative to the extent of the necrosis.
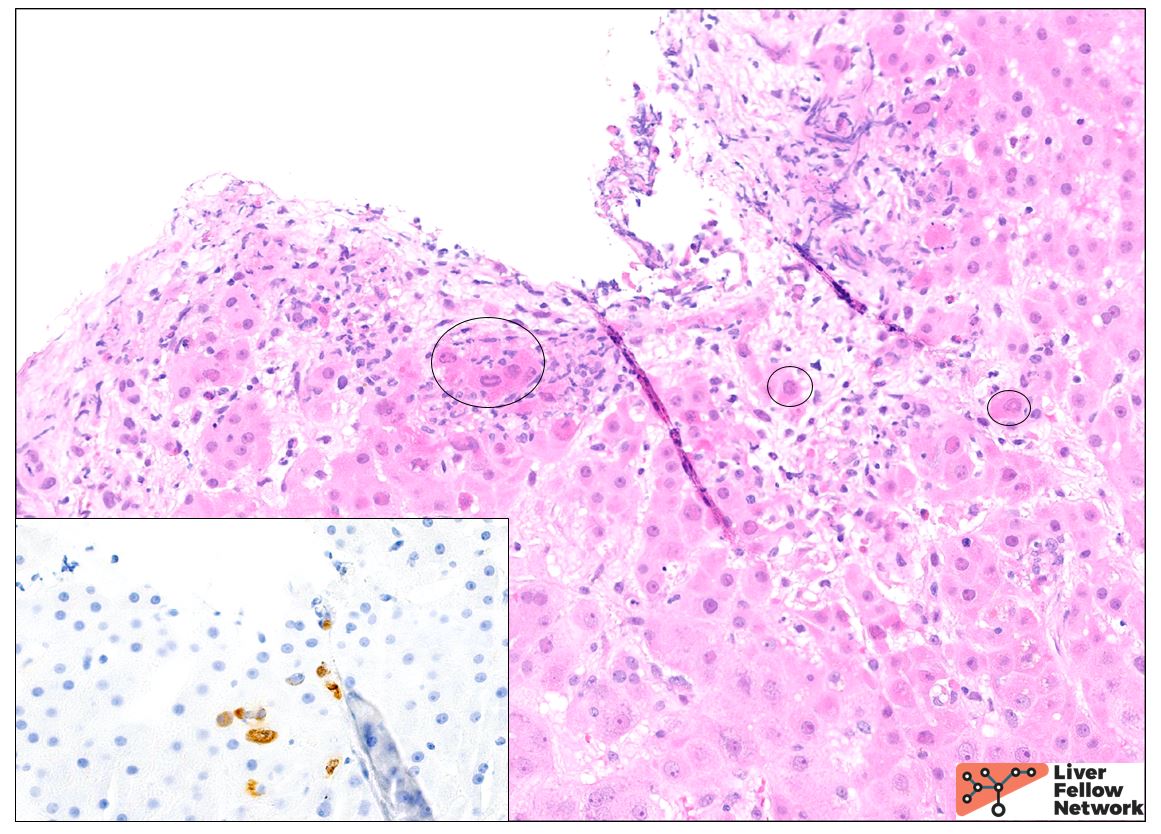
Figure 4. Approximately 3 weeks post-stem cell transplantation for severe combined immunodeficiency (SCID), this patient developed hepatomegaly, transaminitis (AST 100 U/L, ALT 41 U/L), and hyperbilirubinemia (total bilirubin 5.6 mg/dL [conjugated/unconjugated bilirubin values unavailable]). Liver biopsy demonstrates focal necrosis involving several of the portal tracts. “Smudgy” nuclear inclusions are present in several of the adjacent hepatocytes (circled). Rare hepatocytes are highlighted by adenovirus IHC (inset), confirming the diagnosis.
Herpes simplex virus (HSV)-1/2
Herpes simplex virus-1/2 is, as its name suggests, also a member of the Herpesviridae family and a double-stranded DNA virus. HSV hepatitis is exceedingly rare and is typically seen as part of disseminated infection in immunocompromised or otherwise vulnerable populations, such as neonates or pregnant patients, though cases have also been reported in immunocompetent individuals. While reports vary, mucocutaneous findings appear to be present in at least a quarter of cases. Prognosis is grim and timely initiation of antiviral therapy is crucial, with mortality rates of approximately 50% in patients treated with antivirals and greater than 80% in those not receiving treatment. On histology, HSV hepatitis is characterized by crisply delineated (“punched out”) areas of necrosis, in contrast to the relatively ill-defined necrotic foci in adenovirus hepatitis. Again, the viable hepatocytes at the rim of the necrotic focus should be scrutinized for viral cytopathic changes, which in the case of HSV infections classically include chromatin margination (condensation along the periphery of the nucleus), multinucleation, “molding” of adjacent nuclear contours, and Cowdry A (eosinophilic) and/or B (basophilic, “ground-glass”) intranuclear inclusions.
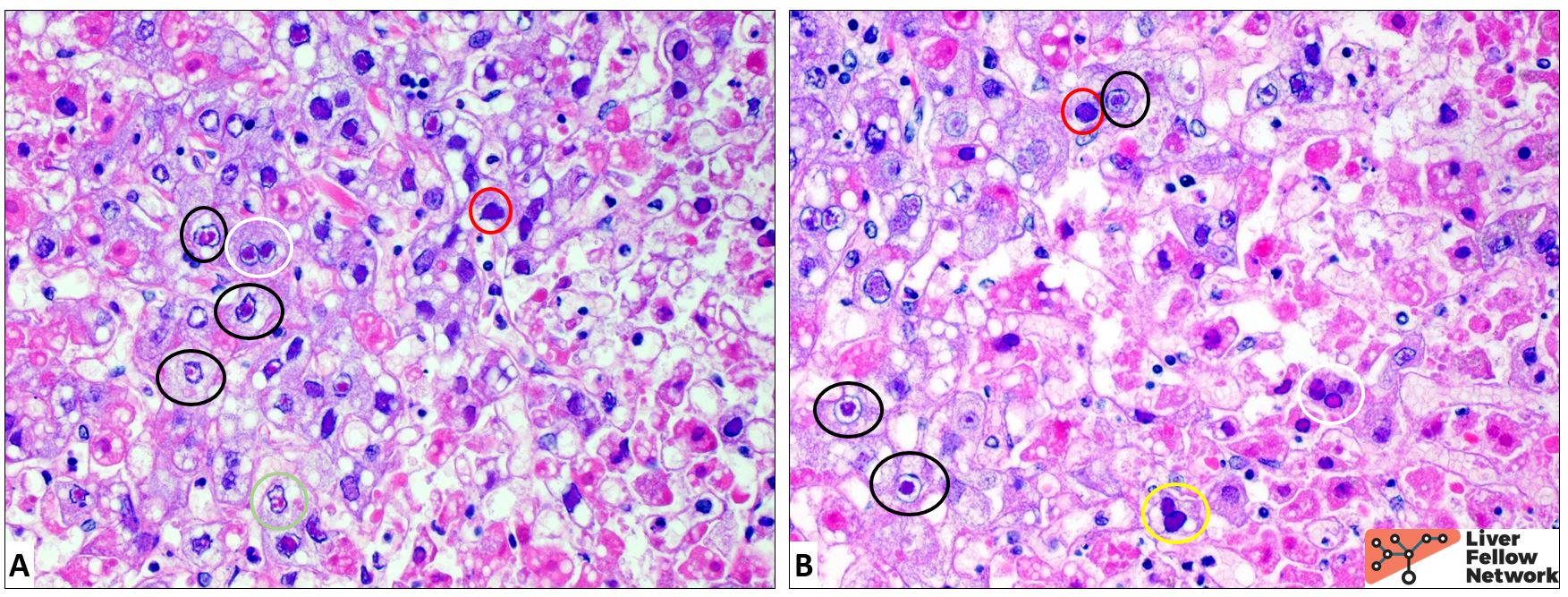
Figure 5. Liver of a neonate with disseminated HSV-1 infection demonstrating classic HSV cytopathic changes, including numerous cells with intensely eosinophilic (“Cowdry A”; black circles) or “ground-glass” (“Cowdry B”; red circles) nuclear inclusions. Multinucleation is also seen (white circles), as is nuclear molding (yellow circle) and chromatin margination in cells without definite inclusions (green circle). The hepatocytes exhibit diffuse cytoplasmic swelling and distortion, a nonspecific sign of injury. Images courtesy of Dr. John Hart, Department of Pathology, University of Chicago Medicine.
Other non-hepatotropic viral hepatitides
While the four agents discussed above represent the most common causes of non-hepatotropic viral hepatitis, other viruses have likewise been linked to acute hepatitis in rare instances. These include parvovirus B19 (also posited to cause chronic hepatitis, though evidence remains limited), typically seen in pediatric patients with systemic parvovirus infections. Histologic findings include extensive necrosis and marked extramedullary hematopoiesis; characteristic “ground-glass” intranuclear inclusions are identified within the hematopoietic cells. In addition, though further investigation is necessary, rare reports of acute hepatitis in the setting of influenza A infection can be found in the literature.
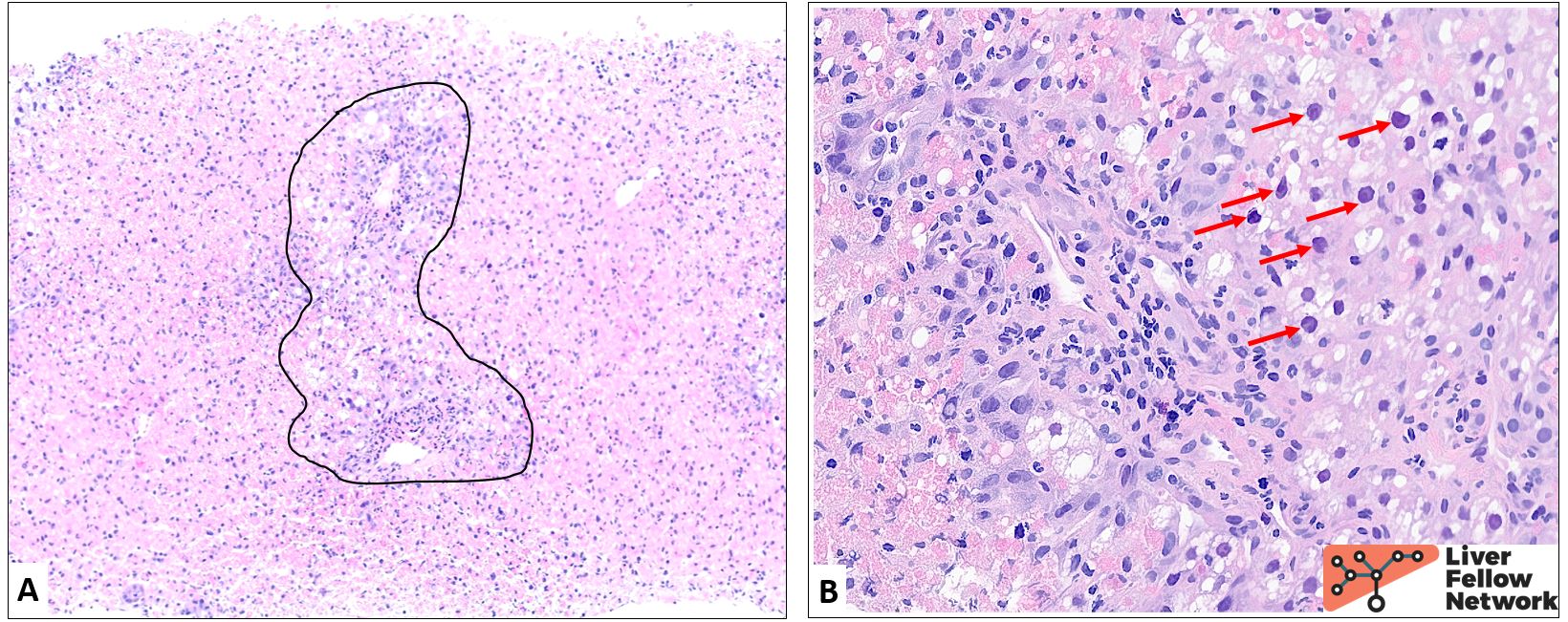
Figure 6. Liver of a patient with influenza A infection.At low power (A), note extensive parenchymal necrosis with relative sparing of periportal hepatocytes (area circled in black). At higher power (B), the viable hepatocytes exhibit diffuse swelling (nonspecific evidence of injury) and the nuclei frequently display viral inclusions or a “sanded” appearance (red arrows). No multinucleated cells or characteristic HSV- or CMV-type inclusions are identified. An adenovirus immunostain is negative. The clinical and pathologic impression in this case supported a diagnosis of fulminant hepatitis due to influenza A.
Conclusion
Though the histologic features may be subtle and viral inclusions are not always present – or may overlap histologically with reactive atypia in hepatocytes or biliary epithelial cells – non-hepatotropic viruses should always be considered on the differential when assessing biopsies from immunocompromised patients. These infections, while rare, may be devastating, and timely diagnosis and appropriate therapy are critical.