Hepatocyte ground-glass pseudoinclusions

Case 1
Clinical history and presentation
The patient is a 75-year-old male with decompensated cirrhosis and known hepatitis B presenting with reactivation of hepatitis B. The patient had not been taking tenofovir for at least three weeks prior to presentation. Past medical history is significant for hepatitis B-related cirrhosis on Viread (tenofovir disoproxil fumarate) and superior mesenteric vein thrombosis on Eliquis (apixaban). Laboratory studies were notable for a total bilirubin of 30.3 mg/dL, alkaline phosphatase of 83 U/L, AST of 1,326 U/L, and ALT of 1,142 U/L. Alpha-1 antitrypsin phenotyping demonstrated an MM phenotype. Toxicology screening was negative. Serologic studies were positive for hepatitis B core antibody and hepatitis B surface antigen, with an HBV DNA level >100,000,000 IU/mL. Testing for hepatitis A, hepatitis C, hepatitis D, and hepatitis E infections was negative. CMV testing was also negative.
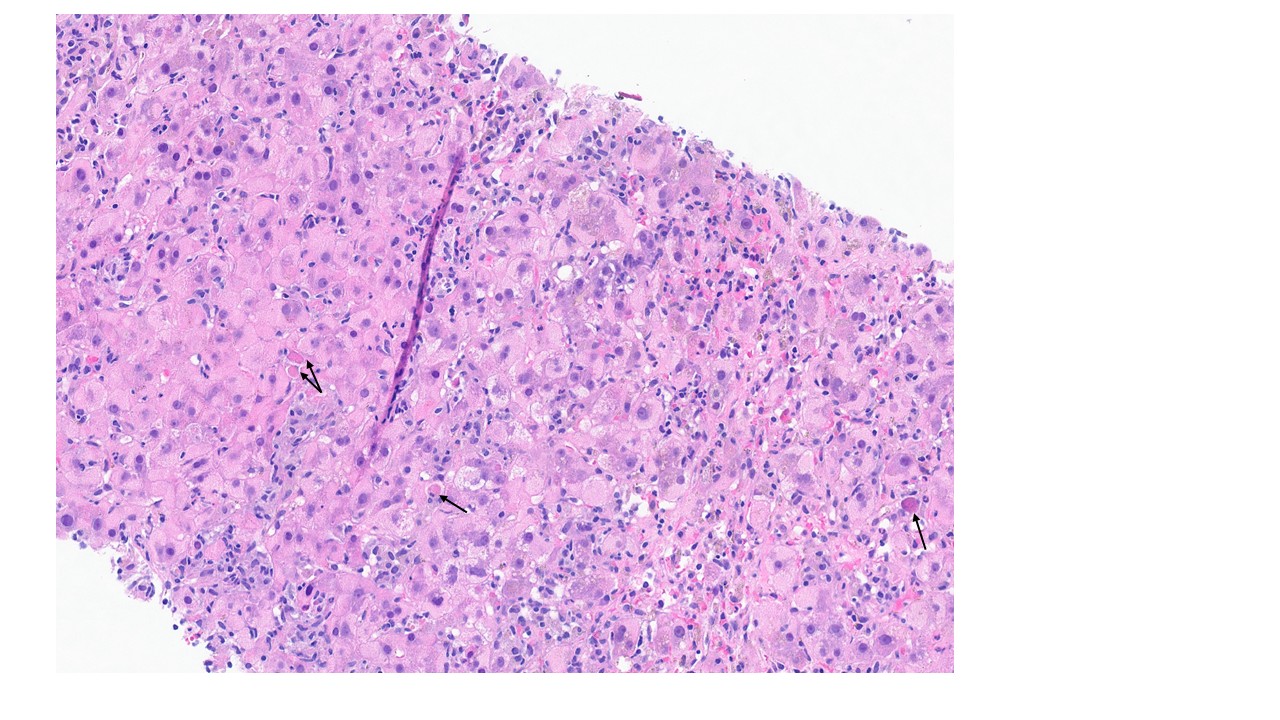
Figure 1. Brisk portal and lobular inflammatory cell infiltrates with interface activity. There is diffuse hepatocyte swelling and cytoplasmic ground-glass change. Acidophilic bodies are also evident (black arrow), and there is mild canalicular cholestasis.
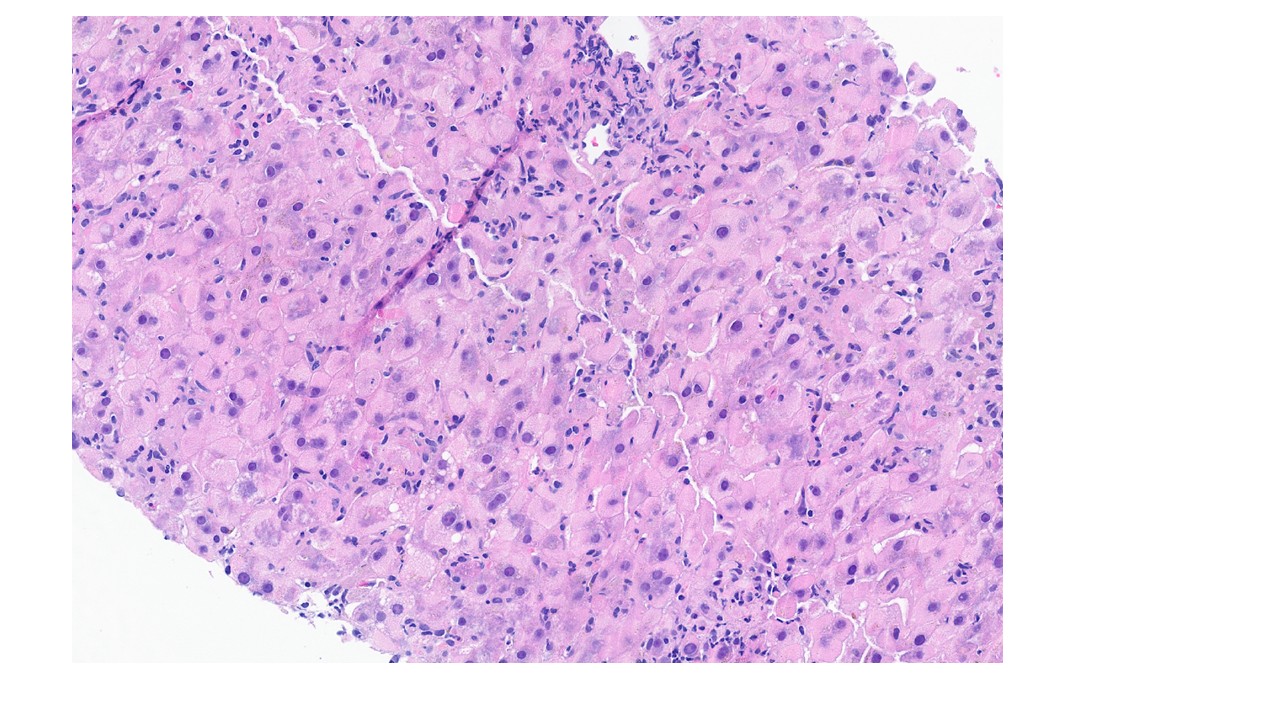
Figure 2. Predominantly lymphocytic infiltrates are present within the lobular parenchyma, with hepatocyte nuclear pleomorphism and diffuse ground-glass changes of the hepatocytes.
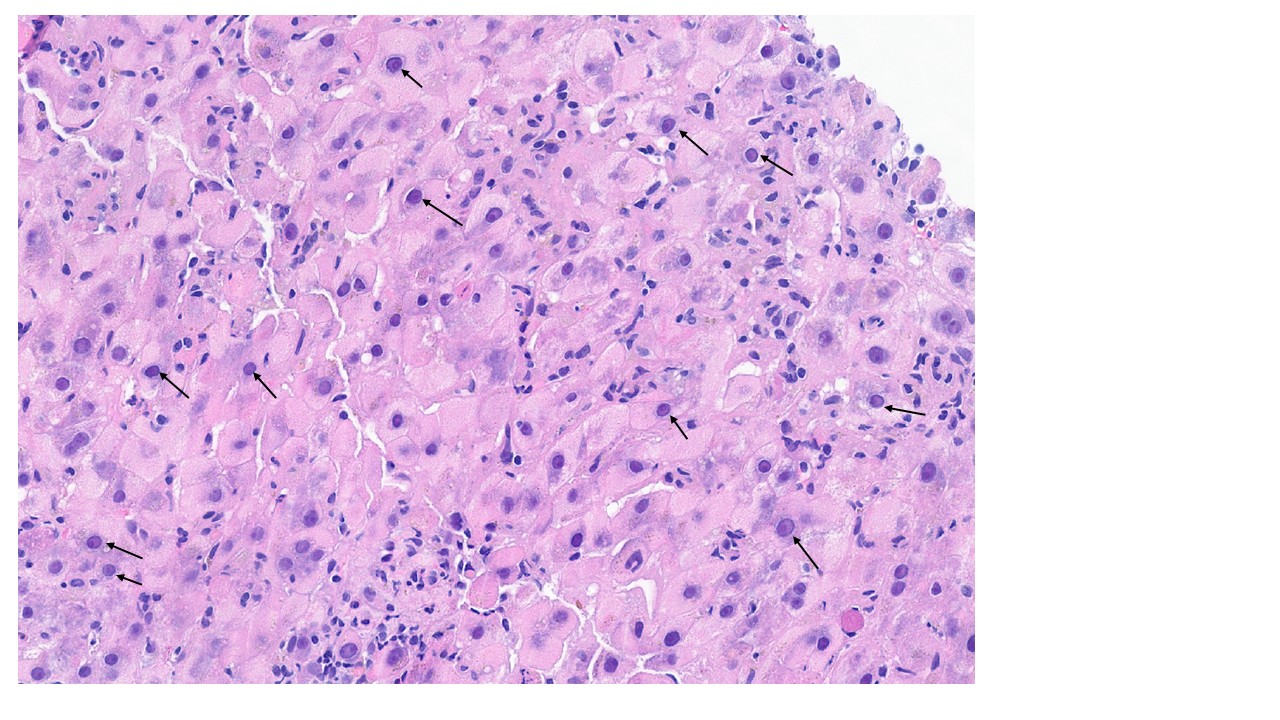
Figure 3. Ground-glass hepatocytes are typically seen in patients with elevated HBsAg levels or active viral replication. Hepatocytes nuclei appear “sanded” due to large amounts of core (black arrow).
Discussion
Ground-glass hepatocytes are a classic histologic hallmark of chronic hepatitis B virus (HBV) infection when hepatitis B surface antigen (HBsAg) is elevated or in active viral replication. Although ground-glass change is not invariably present, its identification on liver biopsy should prompt careful evaluation for HBV infection, particularly in patients with high viral load or chronic disease. Histologically, the cytoplasm of affected hepatocytes appears finely granular, homogeneous and pale eosinophilic on H&E staining. Immunohistochemical staining for HBsAg typically demonstrates cytoplasmic or membranous positivity in chronic hepatitis B, while HBcAg expression may be detected in the nuclei or cytoplasm of hepatocytes, depending on the phase of infection and the degree of viral replication. Although historically ground-glass hepatocytes have been regarded as a characteristic feature of HBV infection, similar pseudoground-glass changes have increasingly been recognized in non-HBV settings, including polypharmacy-associated glycogen accumulation and certain metabolic conditions. Therefore, correlation with serologic studies, immunohistochemistry, and clinical history is essential to distinguish HBV-associated ground-glass hepatocytes from their morphologic mimics. Recognition of this classic HBV-related finding remains important, as chronic HBV infection is a major cause of cirrhosis and hepatocellular carcinoma worldwide and warrants appropriate clinical evaluation and antiviral management.
Case 2
Clinical history and presentation
This 47-year-old male patient with a history of heavy alcohol use and metabolic dysfunction-associated steatotic liver disease (MASLD), type II diabetes, and dyslipidemia is status post heart transplantation in 2008 for complex congenital cardiac malformation. Of note the patient is on multiple medications, including trimethoprim-sulfamethoxazole and tacrolimus.
Laboratory studies are notable for alkaline phosphatase 264 U/L, AST 47 U/L, ALT 42 U/L, and a positive anti-nuclear antibody (ANA) titer. The HbA1c is elevated at 8.8%
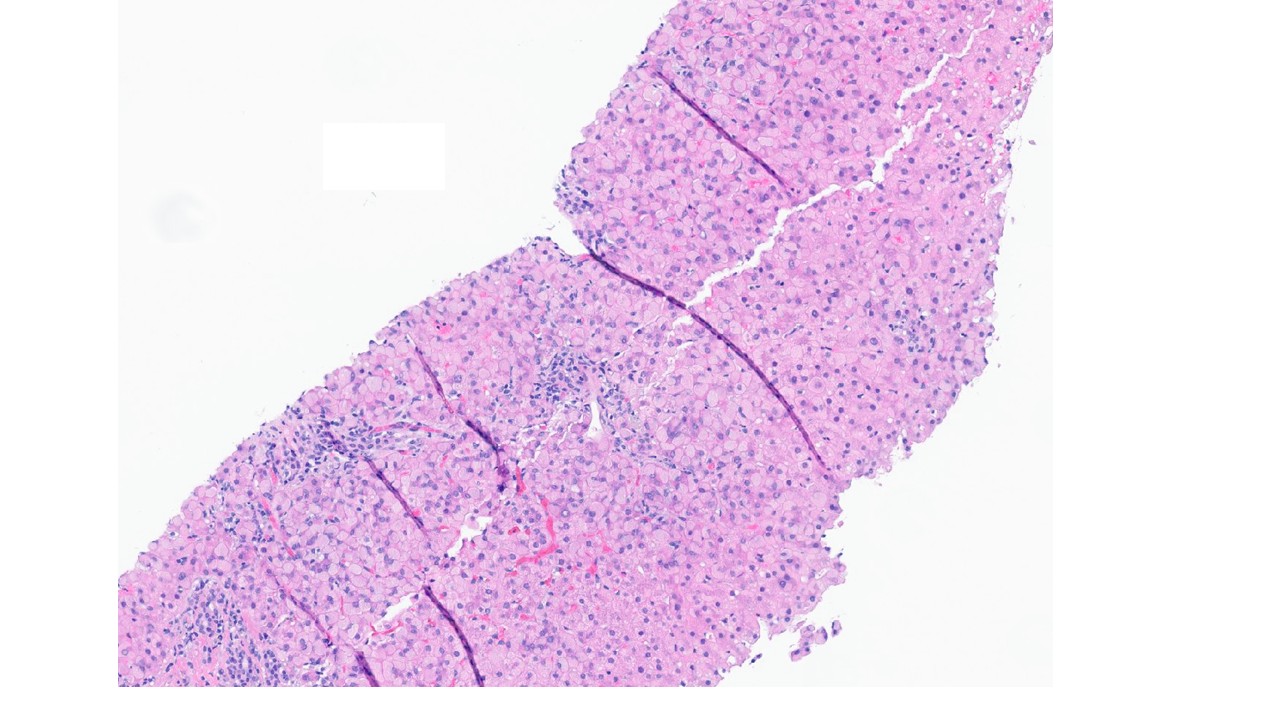
Figure 1. Low-power examination shows diffuse hepatocyte swelling with prominent ground-glass pseudoinclusions.
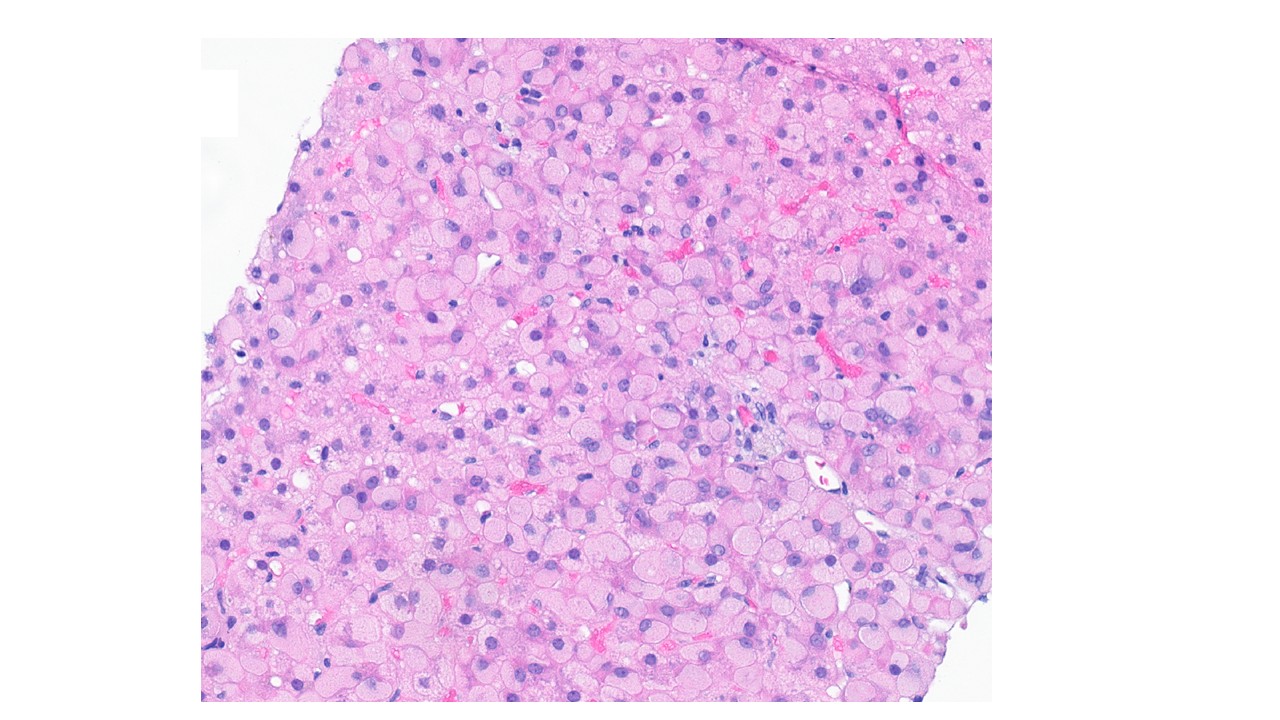
Figure 2. Diffuse hepatocyte swelling with prominent ground-glass pseudoinclusions within hepatocytes.
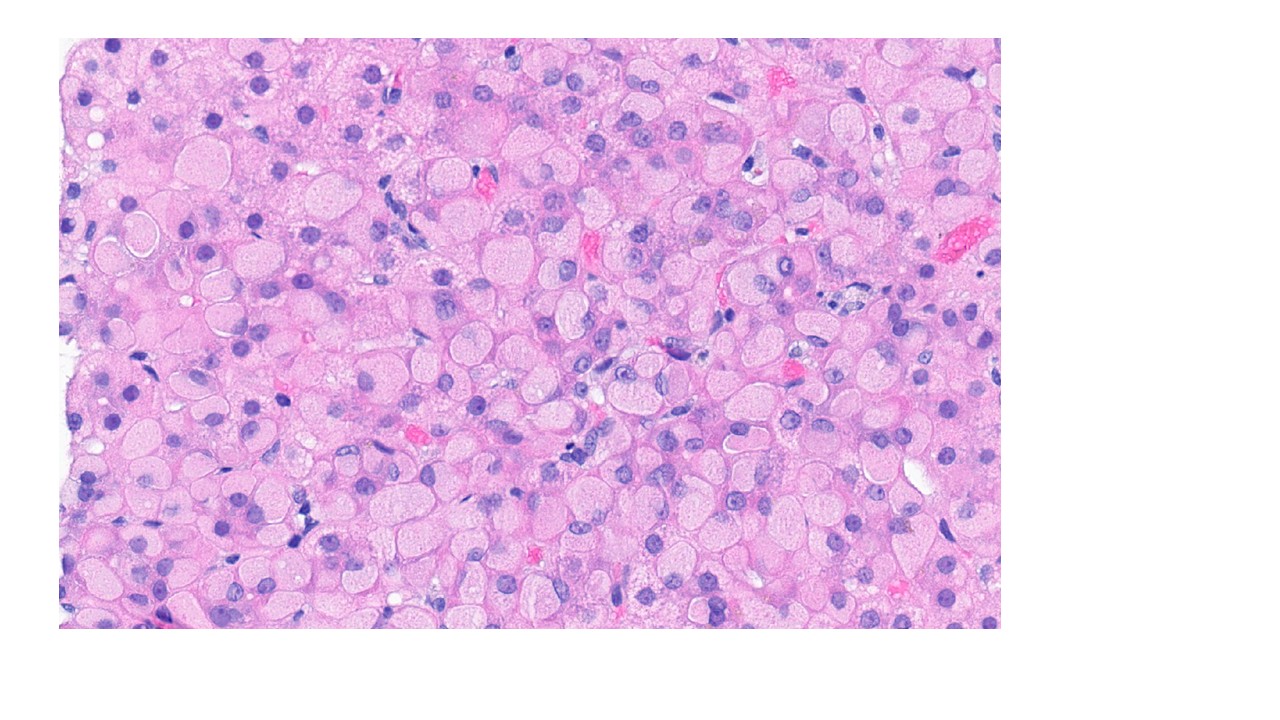
Figure 3. Cytoplasmic ground glass appearance of the hepatocytes, the nuclei are usually located at the periphery of the cell.
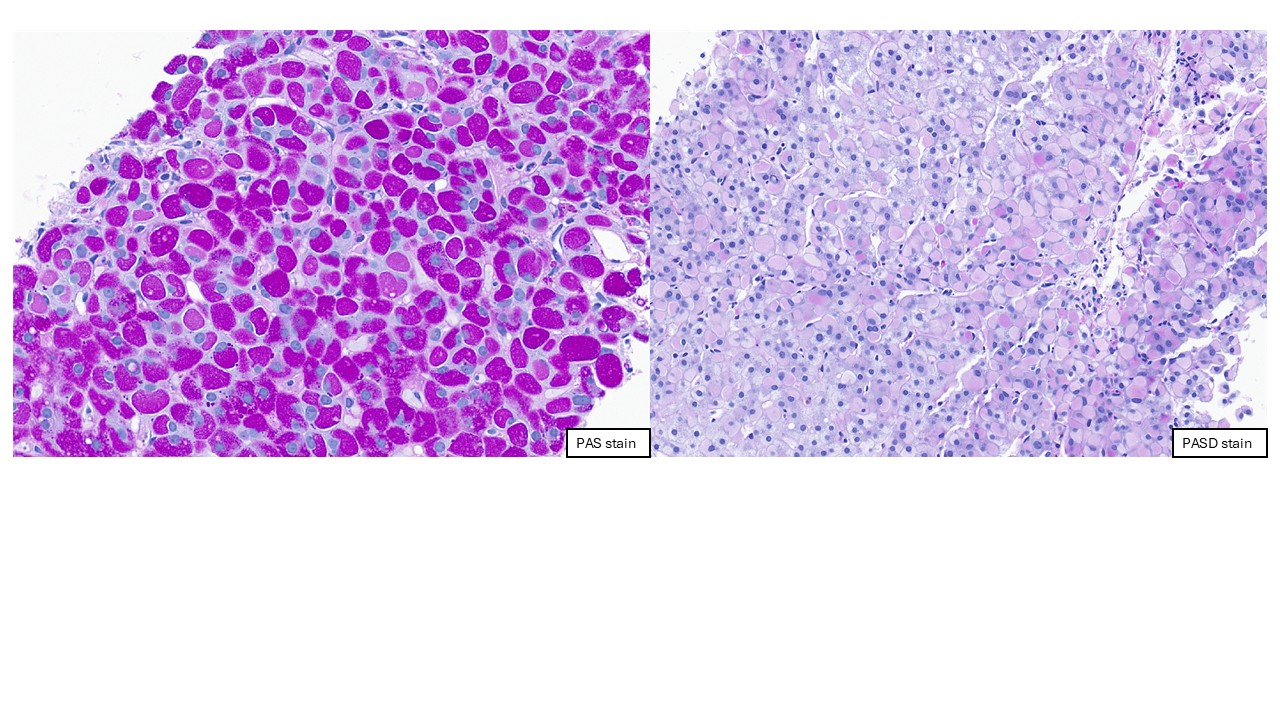
Figure 4. The ground-glass pseudoinclusions are PAS-positive, and most are PASD-sensitive.
Discussion
This patient who is immunocompromised (status post heart transplantation), has been taking numerous medications (polypharmacy) for many years, including warfarin, varenicline, ubrogepant, tacrolimus, trimethoprim-sulfamethoxazole, sodium bicarbonate, sirolimus, senna-docusate sodium, rosuvastatin, rimegepant, propranolol, pregabalin, potassium citrate, polyethylene glycol 3350, pantoprazole, and ondansetron. A liver biopsy was performed to evaluate a mild elevation in transaminases and revealed prominent pseudoground-glass change in hepatocytes. There was no evidence of fibrosis. The presence of comorbid diseases and the numerous medications make it impossible to determine whether the ground-glass pseudoinclusions reflect hepatocyte adaptation or hepatocyte injury. Clinically, individuals with glycogen pseudoground-glass change are almost always immunosuppressed and are taking numerous medications. Given the patient's history of polypharmacy related to heart transplantation, the hepatocyte ground-glass pseudoinclusions are regarded as a manifestation of clinically insignificant drug-induced liver injury.
Case 3
Clinical history and presentation
This patient is a 59-year-old man with a history of buccal squamous cell carcinoma (SCC) diagnosed in 2021, status post chemotherapy and hybrid proton therapy beginning in 2022, who was found to have elevated liver function tests (LFTs) and underwent a liver biopsy. The patient had been taking numerous medications long-term, including ubiquinone/red yeast rice, tramadol, pregabalin, pentoxifylline, levothyroxine, probiotic supplements, hydrocodone-acetaminophen, docusate sodium, diclofenac-misoprostol, chromium, benzonatate, baclofen, atorvastatin, aspirin, and acetylcysteine. LFTs at the time of biopsy included AST 160 U/L and ALT 312 U/L; alkaline phosphatase (ALP) and total bilirubin were within normal limits. Antinuclear antibody (ANA) was positive, whereas anti-smooth muscle antibody (ASMA) was negative.
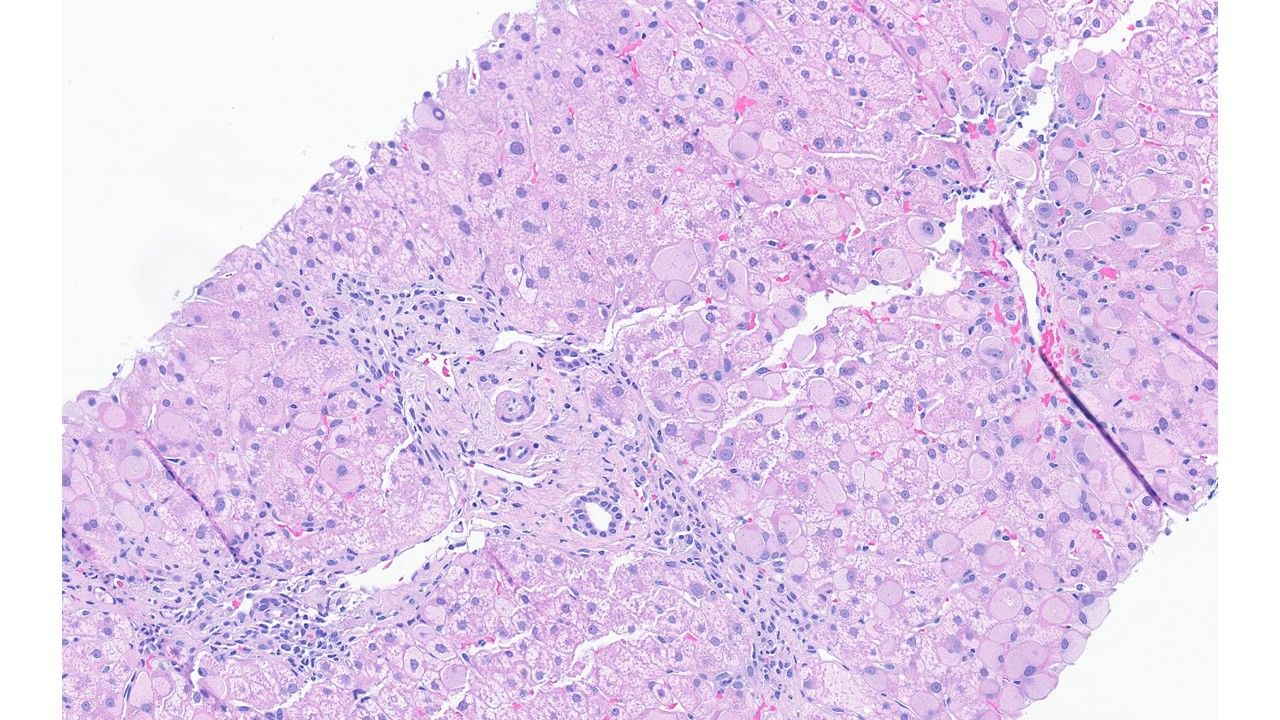
Figure 1. Diffuse hepatocyte swelling with prominent pseudo-ground-glass cytoplasmic inclusions in a non-zonal distribution. There are mild mononuclear inflammatory cell infiltrates in a few portal tracts.
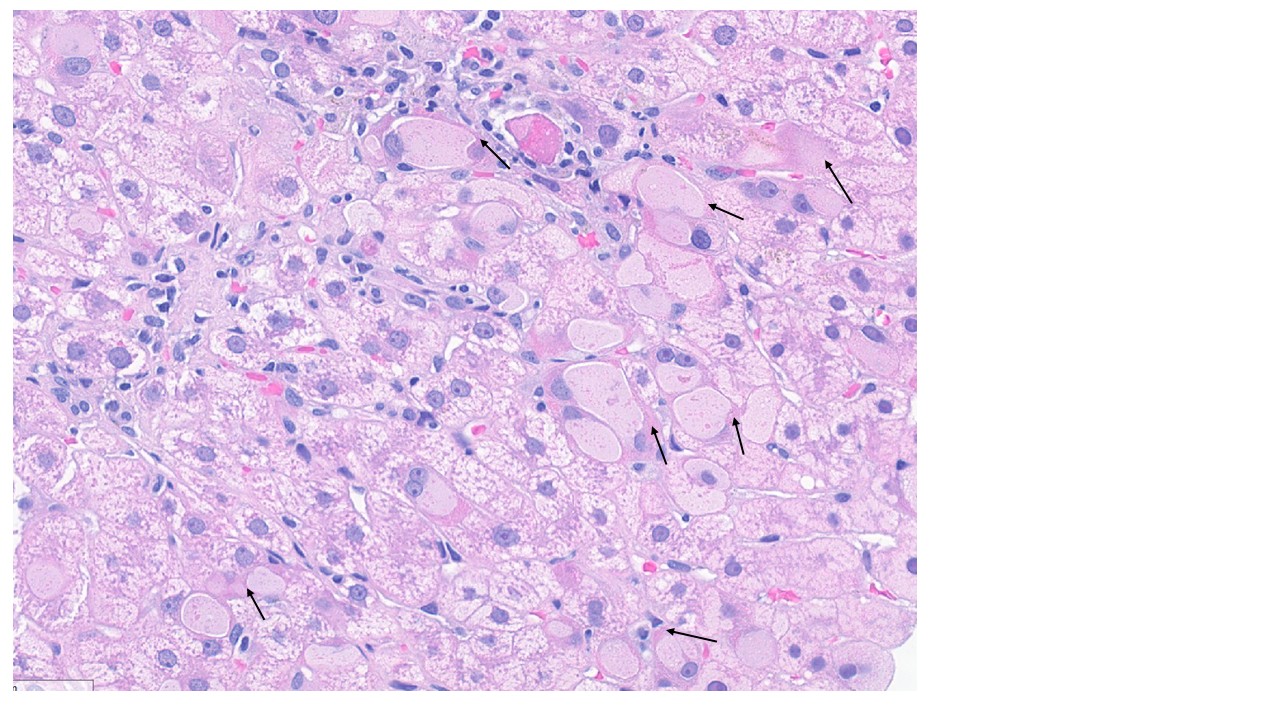
Figure 2. Histologically, the glycogen pseudoground-glass change closely mimics the ground-glass changes that can be seen in chronic HBV hepatitis, with distinct circumscribed gray inclusions surrounded by a rim of normal eosinophilic cytoplasm (black arrow).
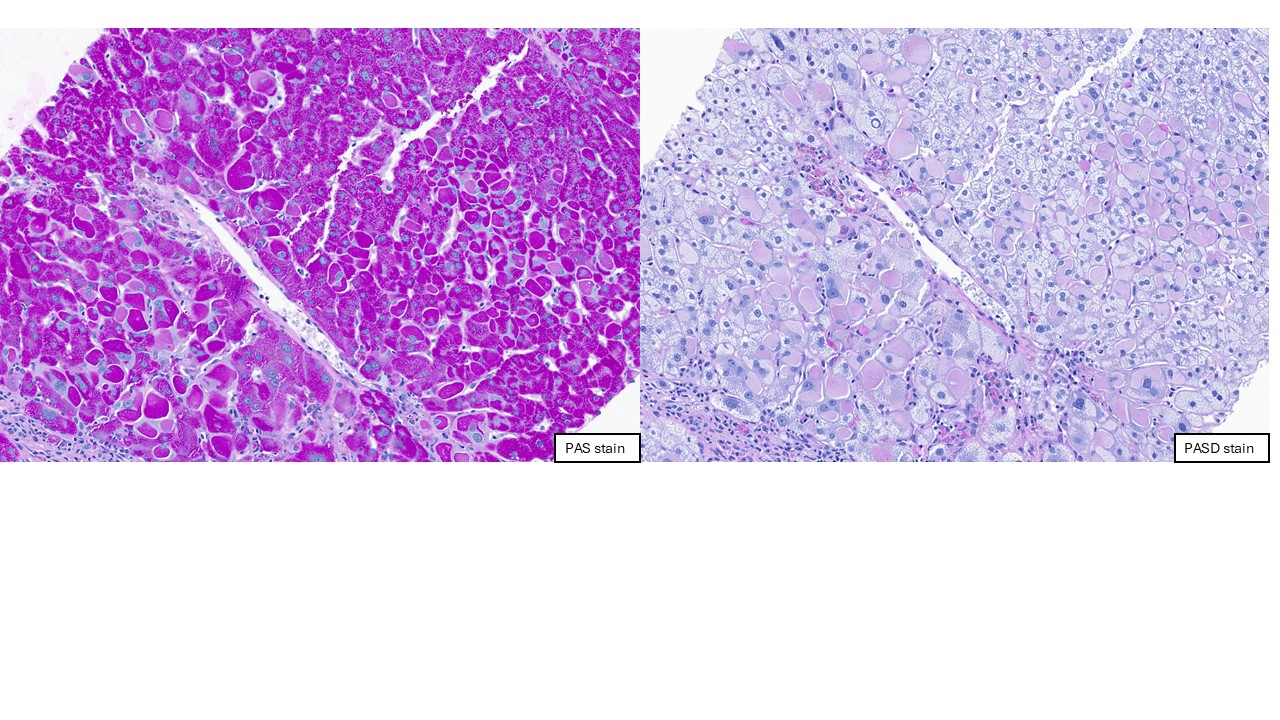
Figure 3. The ground-glass pseudoinclusions are positive on PAS staining, and most of them are sensitive to PASD digestion.

Table adapted from Wisell J, Boitnott J, Haas M, Anders RA, Hart J, Lewis JT, Abraham SC, Torbenson M. Glycogen pseudoground glass change in hepatocytes. Am J Surg Pathol. 2006; 30:1085-90. PMID: 16931952.
Discussion
Classic ground-glass inclusions are a rare finding in liver biopsies, with most cases being associated with chronic HBV hepatitis. Ground-glass intracytoplasmic inclusions can also occur in patients without a history of chronic HBV hepatitis in the setting of polypharmacy, as in our patient with a history of SCC who was taking multiple medications, including Lipitor and Lortab elixir. The proposed mechanism is that polypharmacy leads to aberrant cellular metabolism and abnormal glycogen biogenesis, resulting in the formation of ground-glass inclusions within hepatocytes. This feature is most commonly observed in immunosuppressed patients, particularly those with a history of organ transplantation or underlying malignancies, and who are receiving multiple medications. Recognition of this entity is important to avoid misinterpretation as HBV-related ground-glass change or a glycogen storage disorder, especially when the clinical context supports medication-associated pseudoground-glass change.
Case 4
Clinical history and presentation
A 62-year-old male with a progressive history of paraplegia, peripheral neuropathy, and neurogenic bladder had been diagnosed with adult polyglucosan body disease (APBD) in December 2000. The diagnosis was established through muscle and peripheral nerve biopsies, which showed neurogenic changes and PAS-positive, diastase-resistant polyglucosan bodies within nerve fibers. Subsequent testing confirmed markedly reduced glycogen branching enzyme (GBE) activity in leukocytes and identified a homozygous GBE1 Tyr329Ser mutation by genetic analysis. Recently, the patient was treated for complications of APBD, including a stage IV sacral pressure ulcer, cellulitis, osteomyelitis, and recurrent urinary tract infections. During the hospitalization, he had persistent mild elevations in liver aminotransferase with AST and ALT increased to 111 U/L and 185 U/L and underwent a liver biopsy.
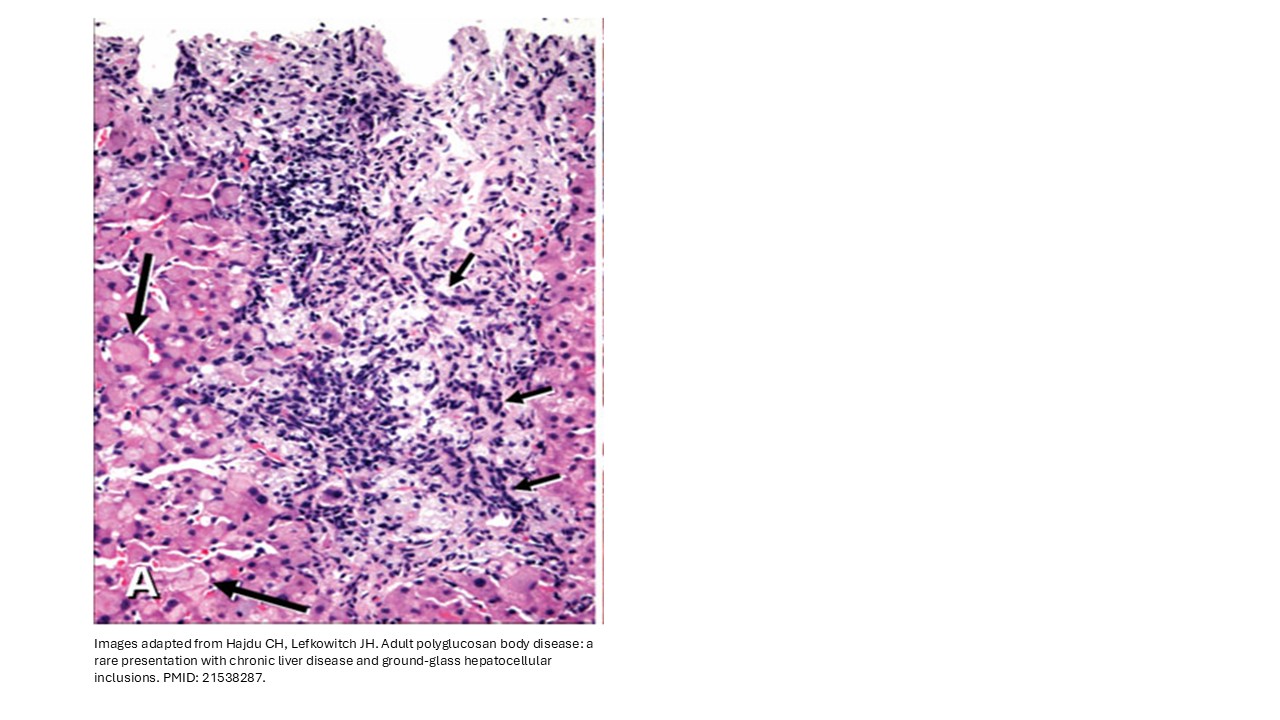
Figure 1A. Polyglucosan bodies with ground-glass appearance (long black arrows) are present in the periportal areas, accompanied by mild portal inflammation (short black arrows).
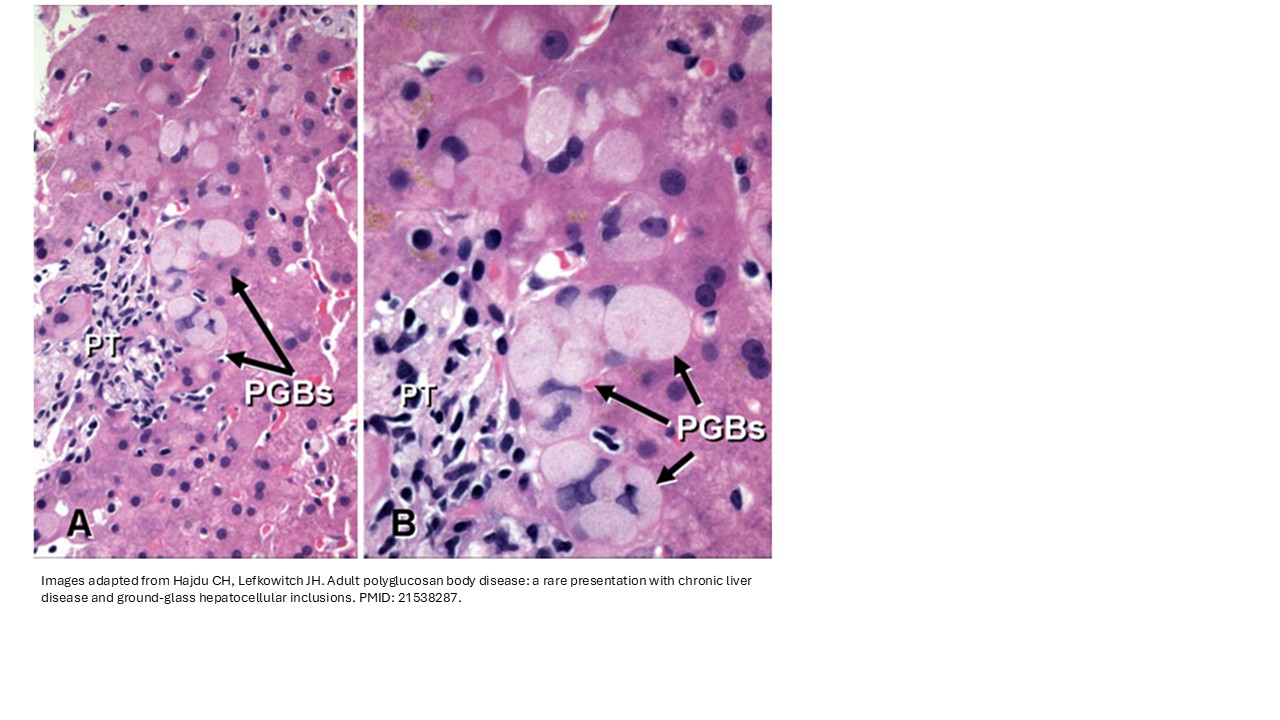
Figure 2A&B. High-power examination showed polyglucosan bodies (PGBs) mimic the ground-glass inclusions seen in hepatitis B. The PGBs are more sharply demarcated within hepatocytes and displace the nuclei to the periphery of the cells.
Discussion
In addition to adult polyglucosan body disease (APBD), ground-glass pseudoinclusions can also be seen in other conditions, including Lafora disease (associated with familial progressive epilepsy, myoclonus, and dementia beginning in childhood), fibrinogen accumulation, uremia, type IV glycogen storage disease, α-1-antitrypsin deficiency, and in chronic alcoholic patients treated with cyanamide to discourage alcohol consumption. Mechanistically, ground-glass change in hepatocytes tends to result from either smooth endoplasmic reticulum proliferation, abnormal glycogen accumulation, or, less commonly, intracellular protein accumulation. Ground-glass hepatocyte inclusions in patients without chronic HBV hepatitis, storage disorders, or cyanamide therapy have been frequently associated with polypharmacy and solid organ transplantation. Based on the available drug histories, no single medication has emerged as a common culprit, suggesting that several drugs may produce similar effects. It also remains unclear why glycogen-associated ground-glass inclusions are more commonly encountered in immunosuppressed patients. Recognition of this rare entity is important for the proper interpretation of this unusual histologic finding and supports polypharmacy as a potential etiology, particularly in patients with a history of transplantation or prior malignancy.
References
1. Wisell J, Boitnott J, Haas M, Anders RA, Hart J, Lewis JT, Abraham SC, Torbenson M. Glycogen pseudoground glass change in hepatocytes. Am J Surg Pathol. 2006; 30:1085-90. PMID: 16931952.
2. Lu HC, González IA, Byrnes K. Ground-glass hepatocellular inclusions are associated with polypharmacy. Ann Diagn Pathol. 2021 Jun;52:151740. Epub 2021 Mar 31. PMID: 33836412.
3. Hajdu CH, Lefkowitch JH. Adult polyglucosan body disease: a rare presentation with chronic liver disease and ground-glass hepatocellular inclusions. Semin Liver Dis. 2011 May;31(2):223-9. PMID: 21538287.
4. Lefkowitch JH, Lobritto SJ, Brown RS Jr, Emond JC, Schilsky ML, Rosenthal LA, George DM, Cairo MS. Ground-glass, polyglucosan-like hepatocellular inclusions: A "new" diagnostic entity. Gastroenterology. 2006 Sep;131(3):713-8. PMID: 16952540.
5. Bejarano PA, Garcia MT, Rodriguez MM, Ruiz P, Tzakis AG. Liver glycogen bodies: ground-glass hepatocytes in transplanted patients. Virchows Arch. 2006 Nov;449(5):539-45. Epub 2006 Sep 22. PMID: 17024424.
6. Li Y, Xia Y, Cheng X, Kleiner DE, Hewitt SM, Sproch J, Li T, Zhuang H, Liang TJ. Hepatitis B Surface Antigen Activates Unfolded Protein Response in Forming Ground Glass Hepatocytes of Chronic Hepatitis B. Viruses. 2019 Apr 25;11(4):386. PMID: 31027244.
7. Bruguera M, Lamar C, Bernet M, Rodés J. Hepatic disease associated with ground-glass inclusions in hepatocytes after cyanamide therapy. Arch Pathol Lab Med. 1986 Oct;110(10):906-10. PMID: 3021086.
8. Elliott EJ, Talbot IC, Pye IF, Hodges S, Swift PG, Tanner MS. Lafora disease: a progressive myoclonus epilepsy. J Paediatr Child Health. 1992 Dec;28(6):455-8. PMID: 1466943.
Acknowledgement
Dr. John A Hart