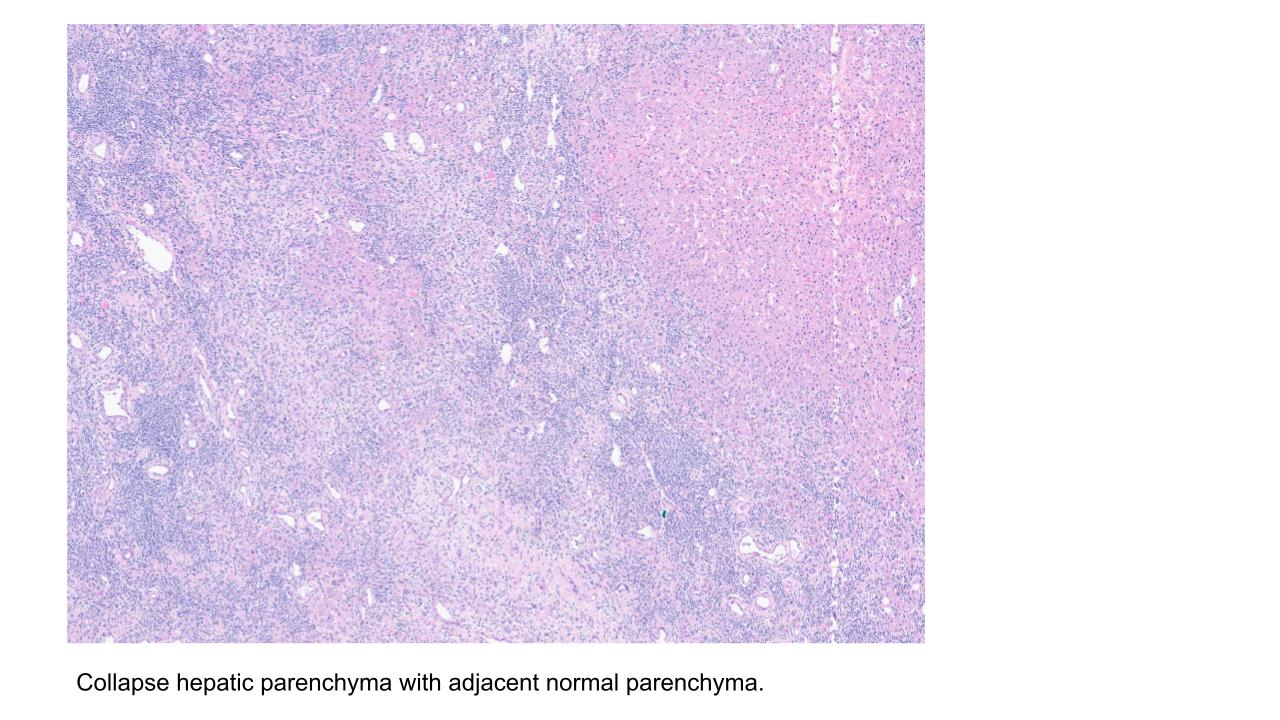
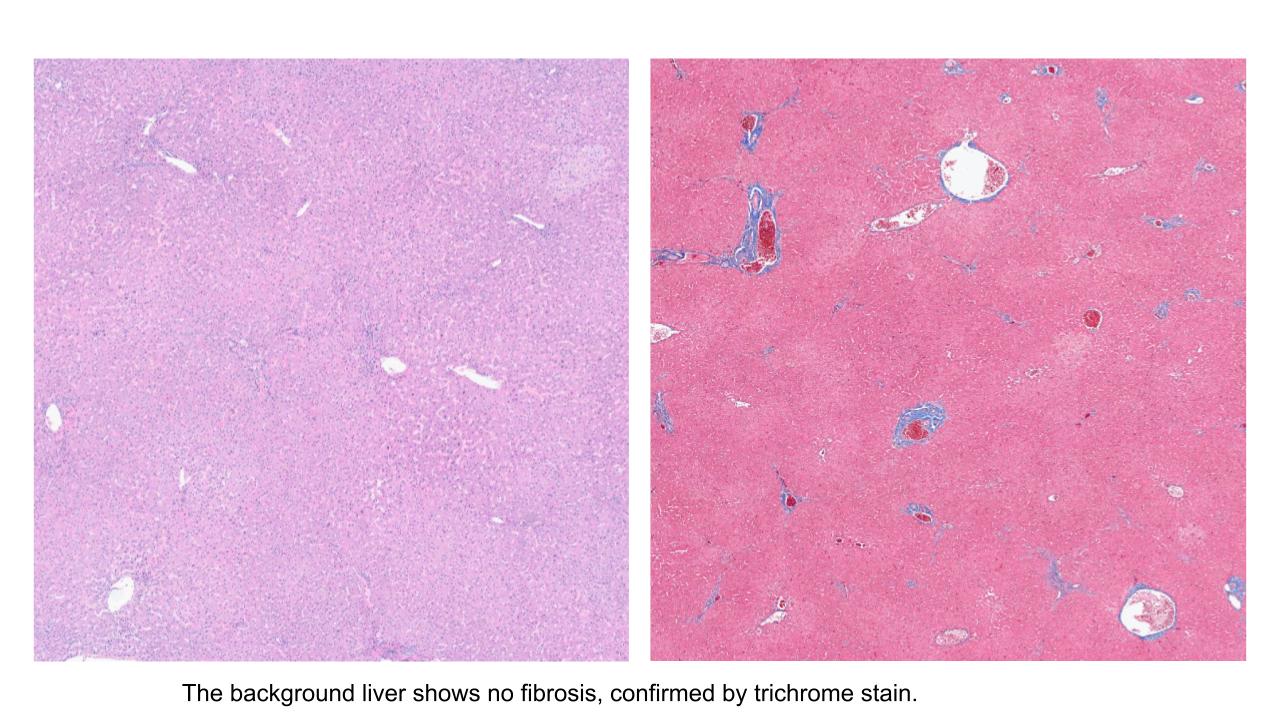
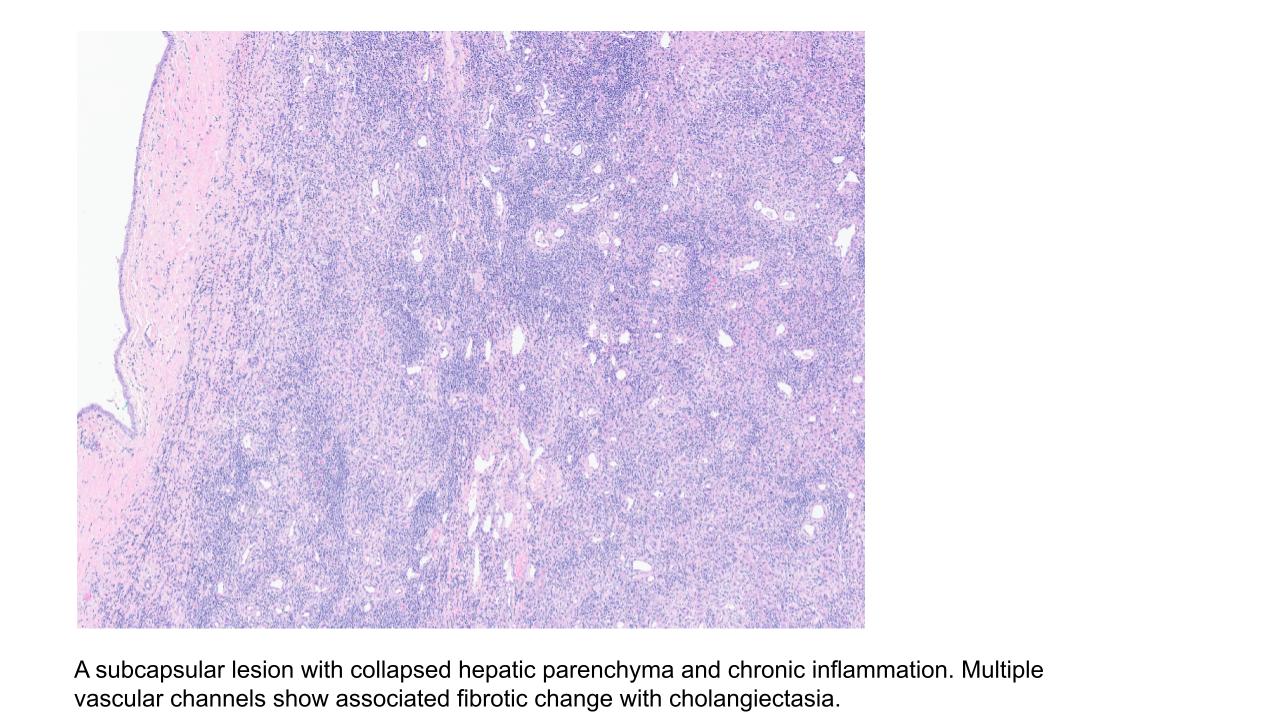
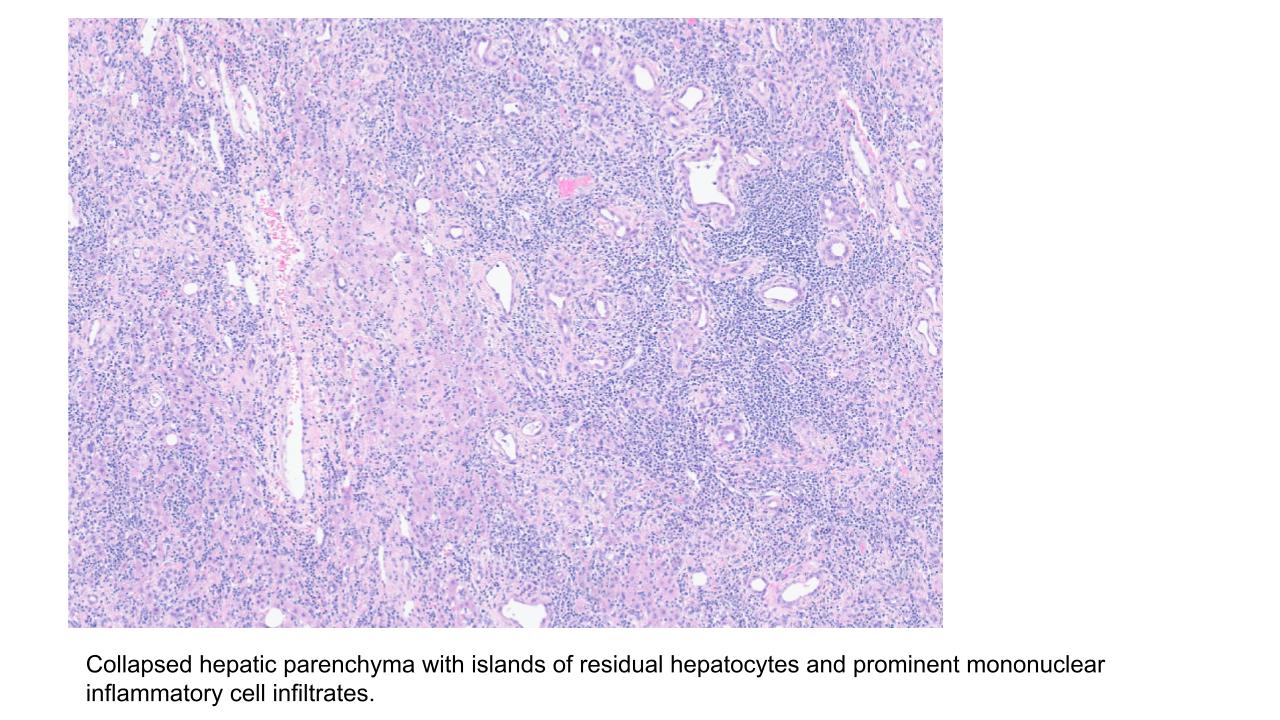
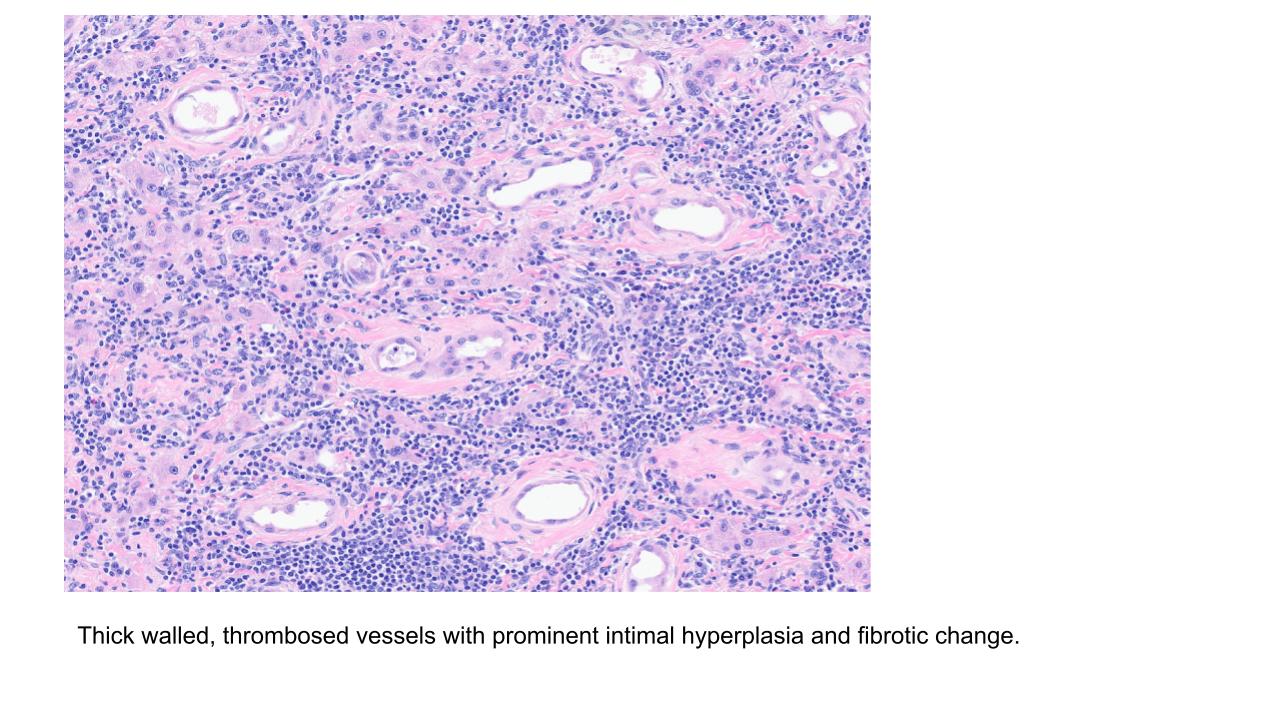
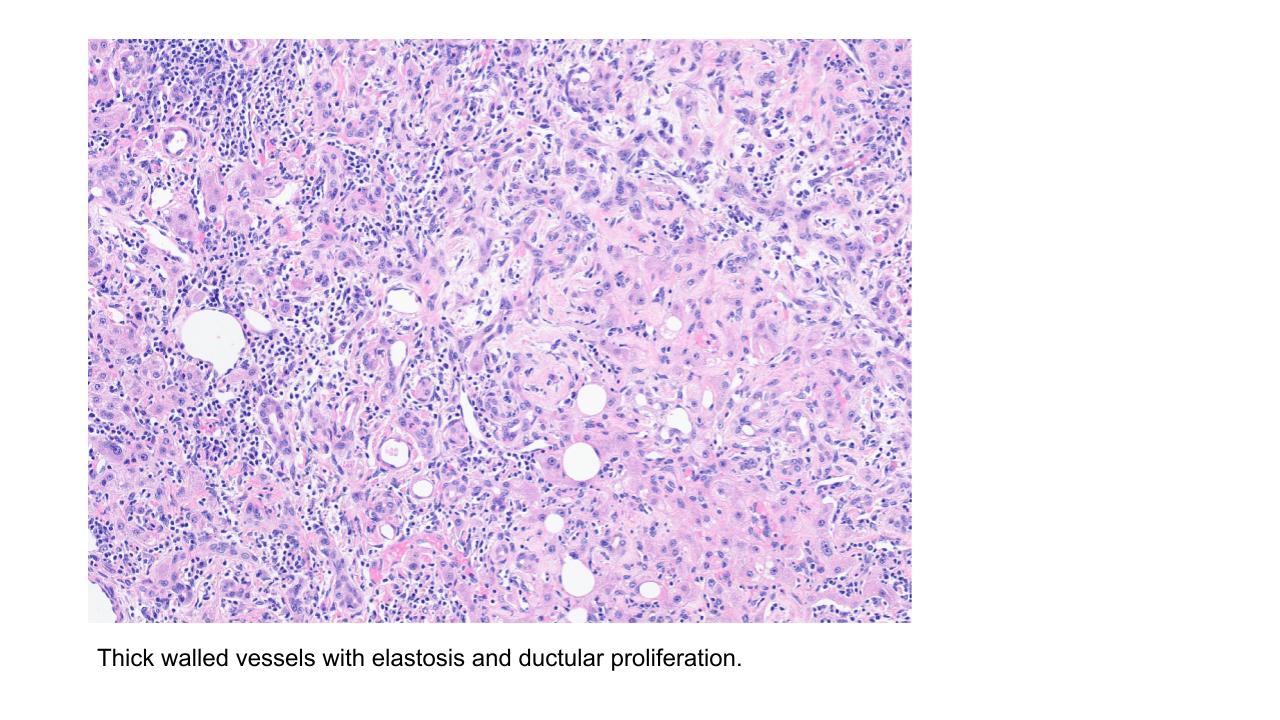
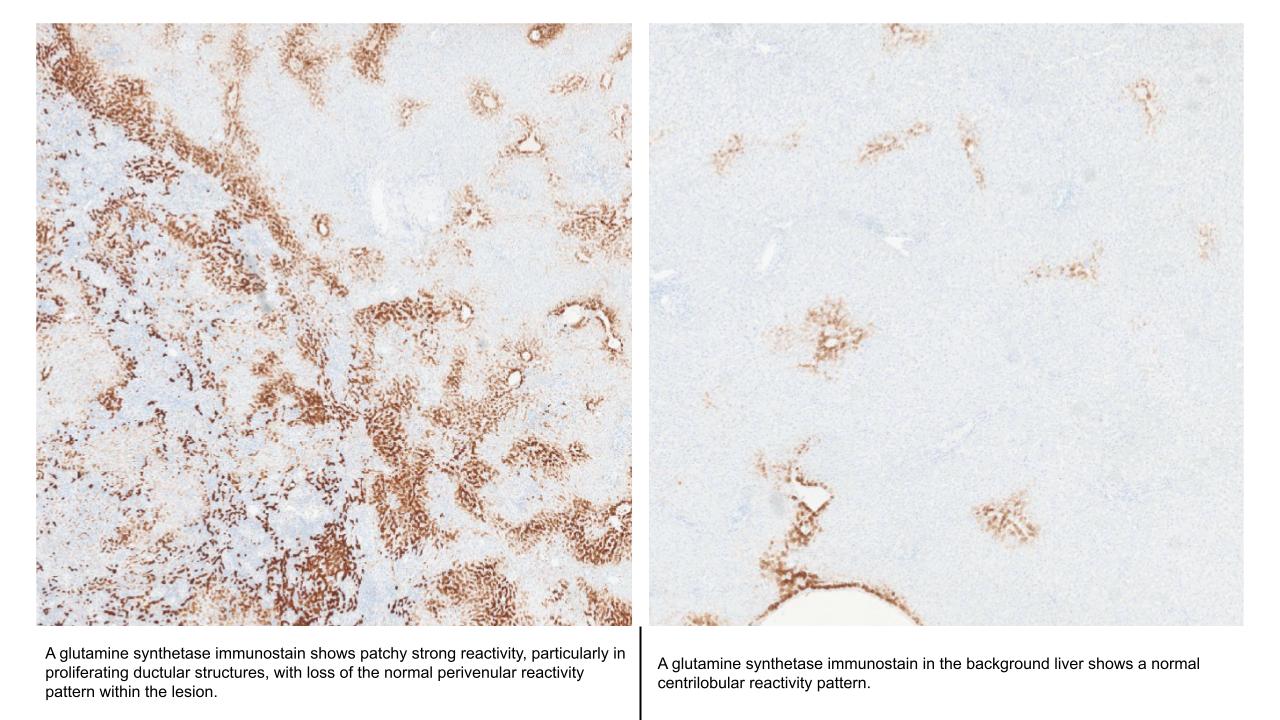
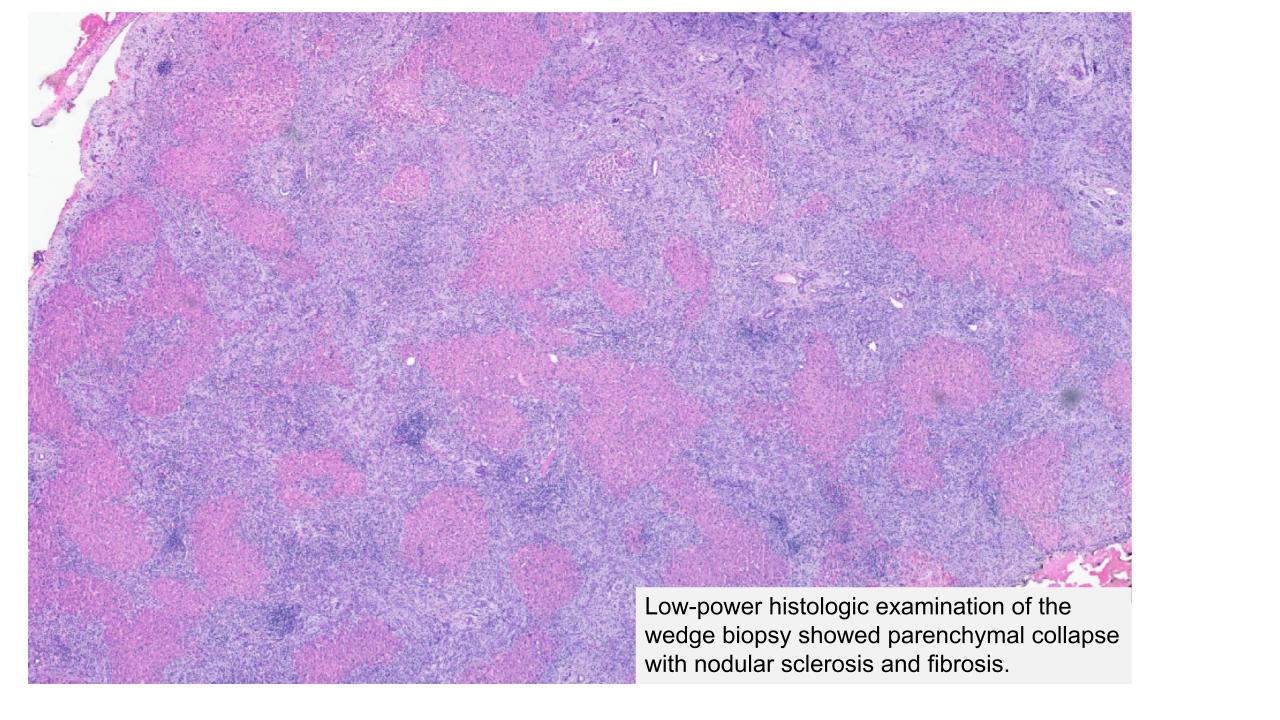
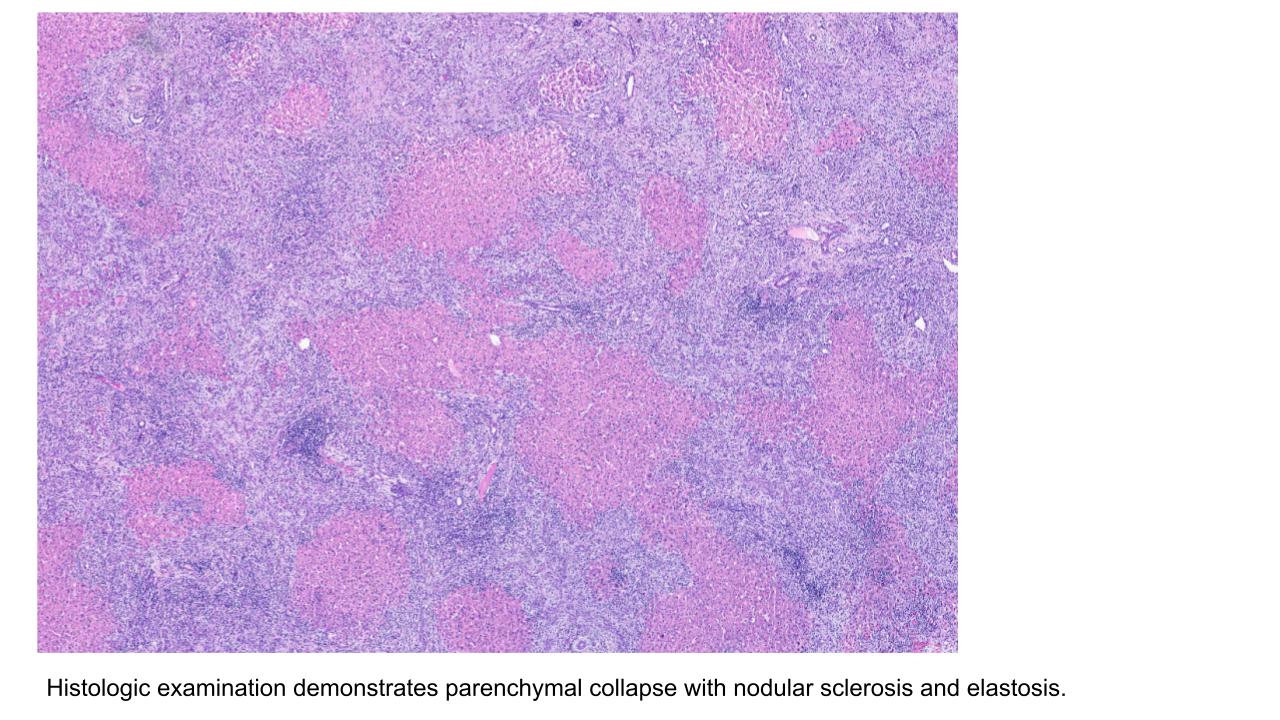
Segmental atrophy

Case 1
Clinical history and presentation
This 48-year-old patient underwent a CT scan revealing an arterial-enhancing, ill-defined hepatic lesion in the right lobe of the liver measuring 4.8 × 4.4 cm, radiologically favored to represent hepatocellular carcinoma (HCC). Liver enzymes were within normal limits. AFP was mildly elevated at 4.8 ng/mL. A segmental resection was subsequently performed.
Case 2
Clinical history and presentation
This patient is a 64-year-old male with a history of choledocholithiasis, status post endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy, followed by cholecystectomy for gangrenous cholecystitis. He recently presented with intermittent, worsening postprandial right upper quadrant pain associated with nocturnal low-grade fevers and night sweats for the past 8 weeks, without weight loss.
Magnetic resonance imaging/magnetic resonance cholangiopancreatography (MRI/MRCP) demonstrated a moderate-sized wedge-shaped area of signal and perfusion abnormality with localized mild ectasia and dilation of the intrahepatic ducts at the anterolateral right hepatic dome, as well as a smaller indeterminate wedge-shaped area in the anterior mid left hepatic lobe. Prior cholecystectomy was also noted.
Computed tomography (CT) of the abdomen showed a dysmorphic liver with right hepatic lobe atrophy and hypertrophy of the caudate and left hepatic lobes, suspicious for cirrhosis. There was interval progression of an ill-defined geographic enhancing lesion involving segments V and VIII, demonstrating indistinct contours with associated intrahepatic biliary ductal dilation and capsular retraction, highly suspicious for intrahepatic cholangiocarcinoma. Circumferential thickening of the extrahepatic bile duct was also present, which may reflect tumor extension or an inflammatory process such as cholangitis.
Liver function tests showed AST 73 U/L, ALT 70 U/L, and total bilirubin 2.2 mg/dL. Alkaline phosphatase was within normal limits. CA 19-9 was elevated at 56.71 U/mL, while AFP was within normal limits.
Discussion
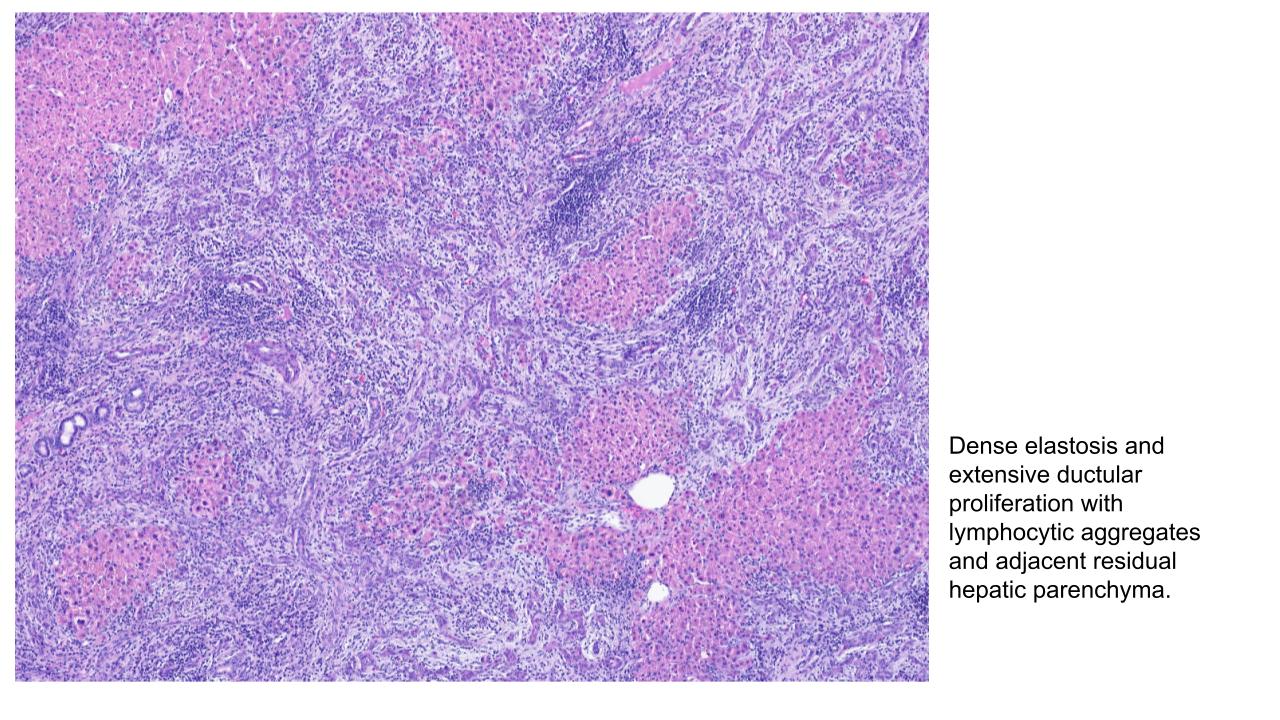
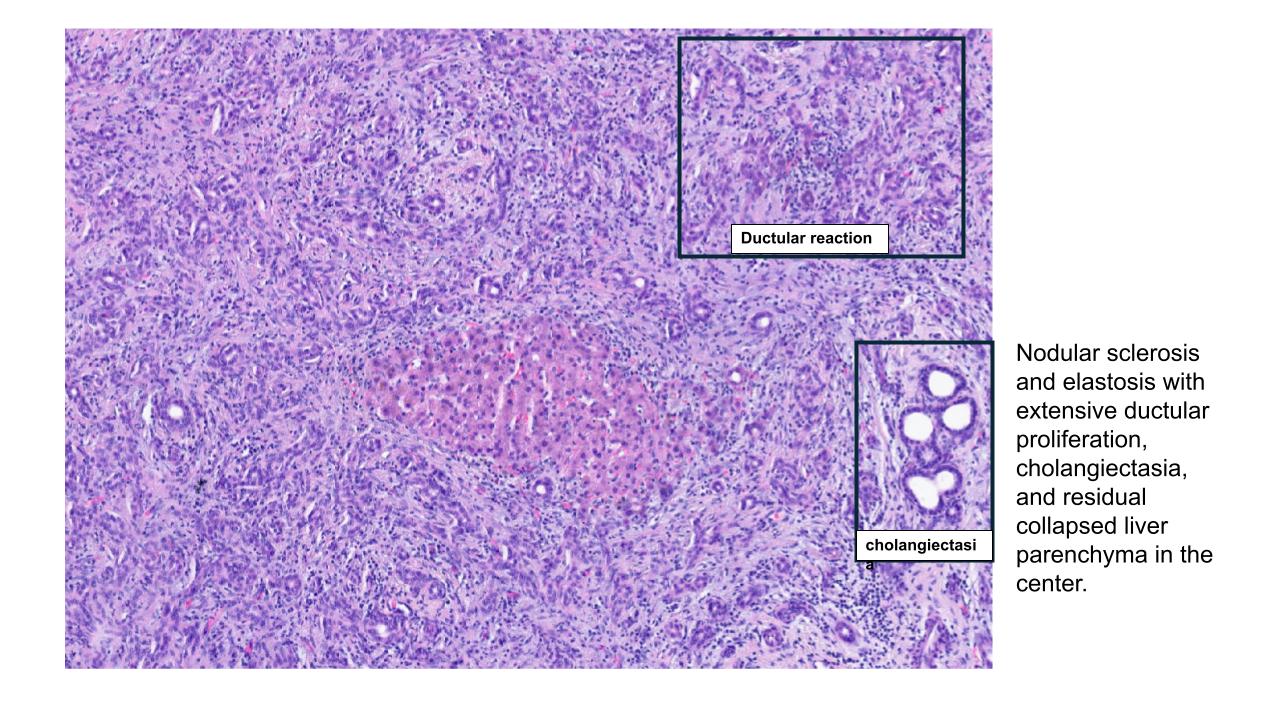
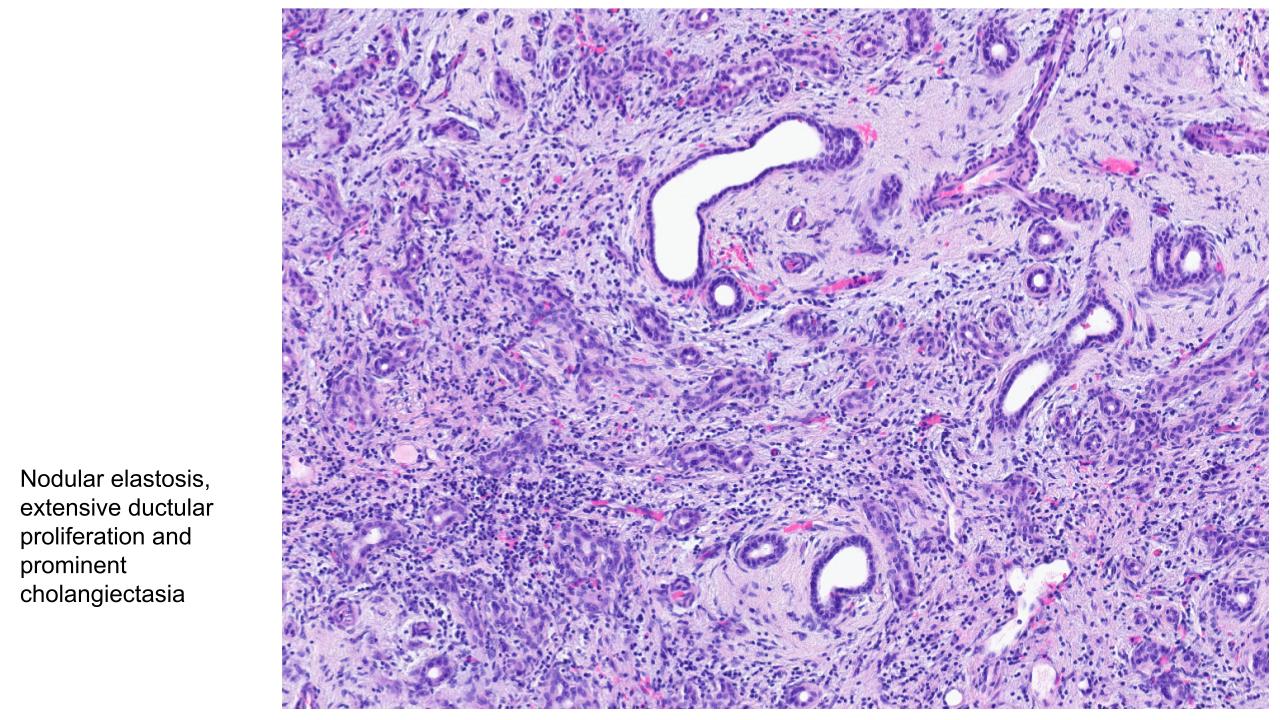
Segmental atrophy of the liver is an uncommon benign pseudotumorous lesion with female predominance characterized by localized loss of hepatic parenchyma with varying degrees of elastotic fibrosis, chronic inflammation, bile ductular proliferation, and vascular abnormalities. The pathogenesis is thought to be related to remote vascular injury or ischemia with subsequent elastin remodeling by liver myofibroblasts, resulting in progressive hepatocellular extinction and parenchymal collapse. It is associated with cardiovascular disease and connective tissue disorders. Radiologically, these lesions may appear as ill-defined hypodense or mass-like hepatic abnormalities with capsular retraction, often mimicking malignant neoplasms such as hepatocellular carcinoma, cholangiocarcinoma, metastatic adenocarcinoma, or scirrhous-type tumors. Histologically, segmental atrophy demonstrates collapsed hepatic parenchyma with islands of residual hepatocytes embedded within dense elastotic or fibrotic stroma, accompanied by chronic inflammation, abnormal thick-walled vascular channels, and variable bile duct proliferation. Advanced lesions may show near-complete loss of hepatocytes with marked elastosis highlighted by Elastic/Verhoeff van-Gieson Stains. Immunohistochemical studies may demonstrate preserved reticulin stain in residual hepatocytes as well as in the background liver with absence of fibrosis, helping to exclude malignancy. Diagnosis requires correlation of radiologic, gross, and histologic findings to avoid overdiagnosis as a primary or metastatic hepatic malignancy. Because imaging findings are often indeterminate, surgical resection is frequently performed for definitive diagnosis, although the lesion itself is benign and prognosis after excision is excellent with no known malignant potential.
Differential diagnosis
- Hepatic sclerosing cavernous hemangioma: Demonstrates vascular channel formation and is less likely to show islands of residual hepatocytes, cystically dilated bile ducts, or abnormally thick-walled vessels.
- Epithelioid hemangioendothelioma (EHE): Composed of poorly vasoformative epithelioid and spindle cells growing in small nests and cords, with intracytoplasmic vacuoles in a background of myxohyaline or fibrotic stroma.
- Cholangiocarcinoma or metastatic carcinoma: Atypical glands are present, the background liver may be cirrhotic in cases of cholangiocarcinoma.
- Hepatocellular carcinoma (HCC): Shows thickened trabeculae with unpaired arteries and reticulin loss, the background liver may be cirrhotic.
References
1. Farsi N et al. Hepatic segmental atrophy: a diagnostic challenge with variable clinicopathologic features and an association with cardiovascular disease. Virchows Arch 2025;487(4):737-743. PMID: 40232381.
2. Hu S et al. Clinicopathologic features of 6 cases of segmental atrophy of liver and review of the literature. Ann Diagn Pathol. 2025;77:152467. PMID: 40101614.
3. Garg I, Graham RP, VanBuren WM, Goenka AH, Torbenson MS, Venkatesh SK. Hepatic segmental atrophy and nodular elastosis: imaging features. Abdom Radiol (NY). 2017 Oct;42(10):2447-2453. PMID: 28456818.
4. Singhi AD, Maklouf HR, Mehrotra AK, Goodman ZD, Drebber U, Dienes HP, Torbenson M. Segmental atrophy of the liver: a distinctive pseudotumor of the liver with variable histologic appearances. Am J Surg Pathol. 2011 Mar;35(3):364-71. PMID: 21317708.
5. Spolverato G, Anders R, Kamel I, Pawlik TM. Segmental atrophy of the liver: an uncommon and often unrecognized pseudotumor. Dig Dis Sci. 2014 Dec;59(12):3122-5. Epub 2014 Jun 7. PMID: 24906695.
Acknowledgements
Dr. John A Hart