Advance Care Planning and Serious Illness Communication

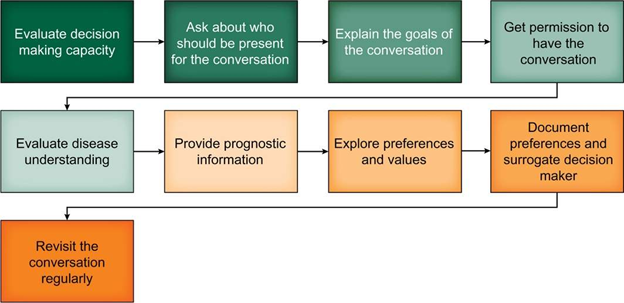
Advance Care Planning (ACP) is a proactive, ongoing, collaborative process of decision making about health care values, goals, and healthcare preferences. It is associated with improved end-of-life outcomes, including satisfaction with care, for serious illnesses. A roadmap for these conversations is shown below, and it spans from helping patients understand their illness to discussing prognosis, values, goals, and preferences, and, finally, documentation. In hepatology, ACP should start at the time of diagnosis of cirrhosis and preferably occur before hepatic decompensations and loss of decision-making capacity.
Reference: Rogal, S., L. Hansen, A. Patel, N.N. Ufere, M. Verma, C. Woodrell, and F. Kanwal, AASLD Practice Guidance: Palliative care and symptom‐based management in decompensated cirrhosis. Hepatology, 2022.
PREPARE is a great website and resource to improve patient engagement with ACP.
With respect to the forms of ACP documentation, below are a few definitions:
| Term | Definition |
| Advanced Directive | Legal document that guides care when a patient is unable to engage in decision-making |
| Living Will | Advanced directives that specify the types of medical care acceptable vs unacceptable to the patient if they cannot communicate |
|
Health care proxy (also known as durable power of attorney for healthcare) |
Identification and documentation of a health care agent by the patient |
| Physician orders for life-sustaining treatment (POLST)/ Medical orders for life-sustaining treatment (MOLST) | Orders signed by a healthcare provider that documents patient preferences about specific treatments (e.g., code status, hospitalization, artificial nutrition) |
Advance Care Planning: Advance Directives for Health Care | National Institute on Aging is an additional resource to better understand these documents.
ACP can take place when patients are healthy or have a stable chronic illness. Serious Illness Communication (SIC) refers to clinician-led supportive communication that should ideally occur as patients get sicker. This includes assessing patients’ illness understanding, sharing prognostic information according to patients’ preferences, exploring patients’ goals, and making recommendations that align with these goals. SIC has been shown to foster trust in providers and improve patient and family satisfaction.
The three core components of SIC include:
- Illness understanding
- Use patients’ preferred languages and take into account health literacy barriers
- Assess patient understanding of disease, using tools such as
- Cirrhosis knowledge questionnaire
- My cirrhosis coach questionnaire
- Cirrhosiscare.ca
- Assess patient understanding of disease, using tools such as
- Prognostic Understanding
- Liver disease often has unpredictable illness trajectories and provider expectations are overly optimistic
- Using prognostic models can help alleviate these barriers
- CTP, MELD 3.0, SALT-M
- Documenting Preferences and Surrogate Decision Makers
- Early identification of health care proxies and discussions about patient values
- Do not carry assumptions about values, preferences, and family structures
- Increased ACP documentation
- Early identification of health care proxies and discussions about patient values
Communication frameworks can provide a path for clinicians to navigate these conversations, which are often difficult. They can assist with delivering serious news, communicating uncertainty, and establishing a plan of care that aligns with patient values. Listed are a few popular frameworks typically employed:
- “Ask-Tell-Ask” simple approach for delivering bad news
- Ask for permission to provide information, and ask what the patient already knows or would like to know more about
- Tell your message in succinct and simplistic language
-
Ask the patient what they think about the information

- “GUIDE” fordelivering serious news (more detail can be found here)
- Get Ready:
- Review the patient’s chart and know the most pertinent core pieces of information (i.e. prognostic information, supporting documentation).
- Ensure the appropriate time and setting along with necessary support (family, friends, trained interpreter) are present.
- Understand what the patient knows:
- Assess how much the patient understands the illness and meet the patient and their caregivers where they are.
- Inform:
- 1-2 sentence headline to succinctly represent the most important information. Avoid medical jargon.
- Demonstrate empathy:
- observe patients’ reactions to news. Acknowledge and respond to their emotions using “I wish” or “NURSE” statements
- Equip the patient for the next step:
- Assess how much the patient is willing to discuss next steps.
- Often, patients are not ready to discuss further issues, and the next step is scheduling another visit.
- When patients are ready, explore what information they may find helpful.
- Use “best case/worst care” frameworks when providing prognostic information to balance hope with realism
- Assess how much the patient is willing to discuss next steps.
- Get Ready:
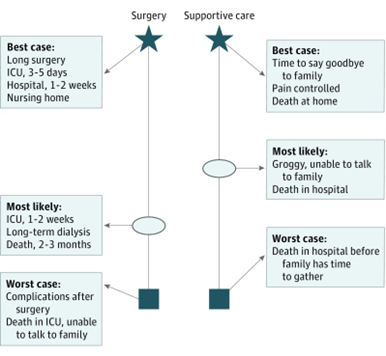
- Best case/Worst Case framework for difficult choices
- Walk patient and loved ones through the best, worst, and most likely outcome of pursuing each treatment option
- Combines shared-decision making with scenario planning
- Walk patient and loved ones through the best, worst, and most likely outcome of pursuing each treatment option
Taylor et al. JAMA Surg. 2017
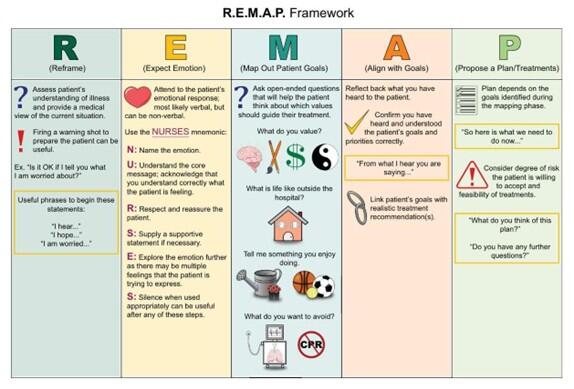
- R.E.M.A.P. framework for more complex goals of care discussions.
- Reframe:
- Assess your patient’s understanding of illness and provide a medical view of the current situation
- Expect emotion:
- Assess your patient’s emotional verbal or nonverbal response.
- Acknowledge and respond to their emotions using “I wish” or “NURSE” statements
- Map out patient goals:
- Ask open-ended questions to help the patient think about which values should guide their treatment
- Align with goals:
- Confirm understanding of patient’s goals and priorities
- Propose a plan:
-
Create a plan that aligns with your patient’s goals
-
- Reframe:
- Serious Illness Conversation Guide framework to guide conversations about prognosis, values, and goals
- Set up the conversation
- Introduce the idea and benefits of the discussion
- Ask permission to have this difficult conversation
- Assess understanding of illness and information preferences
- Evaluate how much information the patient wants to hear
- Share prognosis
- Tailor information to patients’ preferences
- Use phrases such as “I hope” or “I wish” to share realistic optimism
- Use phrases such as “I worry” or “It is also possible…” to acknowledge realistic adverse outcomes or timelines
- Allow for pauses and silences; explore patients’ emotions
- Tailor information to patients’ preferences
- Explore key topics:
- Goals
- Worries
- Activities that provide strength and joy
- Major sources of support
- How much loved ones know
- How much patients are willing to go through
- Close the conversation
- Summarize what you’ve heard
- Make care recommendations
- Affirm commitment to patient
- Set up the conversation
Back to our Case:
Many of the serious illness communication frameworks may be used with Mr. Kwan, who is now here with family after having worsening refractory ascites, weight loss, and immobility. Here are some brief phrases, incorporating the REMAP framework:
Reframe: “The fact that you are needing more paracenteses makes me worried that your liver disease is progressing despite the medications we have tried. In your case, transplant is not an option”
Expect Emotion: “I can’t imagine how scared you must feel. I wish I had better news to share”
Map Out Patient Goals: Given this situation, we want you to feel prepared no matter what happens. Have you thought about how you would like to spend your time if it was cut shorter than you hoped?”
Align with Goals: “I’m hearing that comfort and spendingtime at home with your family are extremely important to you”
Propose a plan: For your ascites, we can consider doing a paracenteses only when the fluid is causing you discomfort, rather than on a schedule. We can also discuss what it may look like to have other procedures, like a TIPS or a long-term drain, that will not cure your disease but make the fluid potentially more manageable for you and your family.
Future Directions
There needs to be a larger emphasis on advance care planning within hepatology, especially early in the disease course before hepatic decompensations or loss of capacity. The AASLD online platform has highlighted several aspects of the guidance and incorporated additional input from experts in gastroenterology, transplant hepatology, nursing, oncology, and palliative care to create a “Palliative Care and Advanced Liver Disease” course (available on AASLD Liver Learning).
The course includes 8 modules ranging from “Introduction to PC for Individuals with Decompensated Cirrhosis”, “Advanced Care Planning and Serious Illness”, to “Liver transplantation and Palliative Care”. Course modules are intended for a broad range of trainees and specialists, with some modules targeted towards specialist palliative care teams. To learn more about the role of palliative care in hepatology, check out our post on palliative care in advanced liver disease.
All hepatology care team members should feel comfortable having serious illness communications to best provide care that aligns with patients’ values, goals, and preferences. Our ability to navigate these conversations can be improved through the AASLD Palliative Care and Advanced Liver Disease course in addition to interventions such as structured observations and simulated clinical scenarios.