Drug Induced Liver Injury with Tuberculosis Treatment

A 12-year-old boy with no significant past medical history was recently diagnosed with sputum positive pulmonary tuberculosis and has been receiving isoniazid, rifampin, pyrazinamide, and ethambutol for 6 weeks. He presents for a routine follow-up visit with infectious disease. He has no acute complaints or symptoms, and his physical examination is unremarkable. His BMI is normal.
Prior to starting the treatment regimen, his baseline labs including liver enzymes, bilirubin, liver and kidney function were all normal. Routine screening labs at follow-up show:
- AST: 220 U/L (normal < 40 U/L)
- ALT: 250 U/L (normal < 40 U/L)
- Alkaline phosphatase: 129 IU/L (normal 25 - 100 U/L)
- Total Bilirubin: 1.2 mg/dL (normal 0.1 - 1.0 mg/dl )
- INR: 1 (normal 0.8 - 1.1)
There is no family history of liver disease, and additional testing for other causes of hepatitis is negative including viral hepatitis (hepatitis A, B, C, D, & E), EBV and CMV testing. Autoimmune testing (ANA, anti-LKM, anti-SM, and total IgG) is negative. Ceruloplasmin is normal. Additional testing for thyroid disease, celiac disease, and CK level are normal. Liver ultrasound is normal making structural or biliary causes of liver enzyme elevation unlikely.
What is the most appropriate next best step in management?
A. Perform liver biopsy
B. Review if any of the medications in his regimen have an association with hepatotoxicity
C. Continue monitoring liver enzymes on repeat labs in 2 weeks
Answer: B
Elevated transaminases in a child receiving multi-drug therapy should prompt a broad differential. Viral, autoimmune, metabolic, and obstructive causes must be systematically excluded through targeted labs and imaging. If a clear etiology is not able to be identified on initial labs/imaging and if the timing aligns with known hepatotoxicity medications the patient is receiving, drug induced liver injury (DILI) becomes increasingly likely.
In this patient, the constellation of normal bilirubin, isolated transaminase elevation, and lack of clinical symptoms, along with recent initiation of multiple potentially hepatotoxic medications should prompt consideration of DILI. Other causes such as viral and autoimmune hepatitis and Wilson disease have been ruled out with the labs above and liver imaging was normal ruling out biliary obstruction or any other vascular abnormality. Until any hepatotoxic drug exposures have been excluded, a liver biopsy would not be the next best step. Medication review and identification of hepatotoxic risk should precede invasive testing.
Liver biopsy is not routinely required for diagnosis of DILI but may be considered in atypical or unresolved cases. If a liver biopsy were performed in DILI, histopathology may show hepatocellular necrosis, lobular inflammation, ballooning degeneration, cholestasis, or mixed hepatocellular-cholestatic injury, depending on the drug and injury pattern.
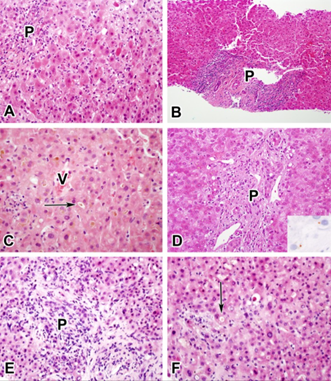
Image 1. Examples of the five most common injury patterns. (A) Acute hepatic injury resulting from ciprofloxacin. (B) Chronic hepatic injury resulting from isoniazid. (C) Acute cholestatic injury resulting from an anabolic steroid. (D) Chronic cholestatic injury resulting from amoxicillin-clavulanate (inset shows positive copper stain). (E and F) Cholestatic hepatic injury resulting from duloxetine. For orientation, P indicates portal area, V indicates central vein, and arrows indicate canalicular cholestasis.
Current American Thoracic Society (ATS) and international DILI guidelines recommend holding hepatotoxic ATT drugs when ALT ≥5 the upper limit without symptoms or ≥3 the upper limit with symptoms or bilirubin elevation. In our patient, the ALT and AST are both greater than 5 times the upper limit of normal raising suspicion for a DILI.
When DILI is suspected, a structured causality assessment should be performed in addition to clinical and laboratory evaluation. Validated tools such as the Roussel Uclaf Causality Assessment Method (RUCAM), also referred to in updated form as RECAM, provide a standardized, semi-quantitative framework that incorporates timing of drug exposure, course of liver enzyme abnormalities after drug withdrawal, risk factors, exclusion of alternative causes, known hepatotoxic potential of the drug, and response to rechallenge. Use of RUCAM/RECAM improves objectivity and reproducibility in attributing liver injury to a specific medication. In parallel, authoritative drug safety resources such as the NIH LiverTox database should be consulted to review established hepatotoxicity profiles, likelihood scores, clinical patterns of injury, and published case data for suspected agents, including first-line anti-tubercular drugs. Integrating structured causality scoring with curated hepatotoxicity databases strengthens diagnostic confidence and supports evidence-based decisions regarding drug withdrawal and stepwise reintroduction. RUCAM remains the most widely used structured causality assessment tool in DILI research and clinical reporting.
In this case, the anti-tubercular therapy (ATT) regimen the patient was started on may be associated with hepatotoxic injury. Incidence of ATT-associated DILI ranges between 2-33%. Several studies emphasize multiple risk factors for this association particularly in the vulnerable pediatric population, such as female gender, poor nutrition, and pre-existing liver disease.
After diagnosing the patient with a drug induced liver injury (DILI), what would be the next best step in medication management?
A. Continue all four ATT medications since the child is asymptomatic
B. Add non-hepatotoxic medications and continue the current regimen
C. Discontinue isoniazid, rifampin, and add streptomycin
D. Stop all anti-tubercular medications immediately and restart after 2 weeks
E. Discontinue isoniazid, rifampin, and pyrazinamide.
Answer: E
Tuberculosis is still a significant public health concern, particularly in South-East Asia and India, so this child requires effective treatment of the disease. The primary intervention in ATT-related DILI involves discontinuing all potentially hepatotoxic drugs like isoniazid, rifampin, and pyrazinamide. This step is critical to prevent further liver injury, especially given the established association between anti tubercular therapy induced liver injury.
After discontinuation of hepatotoxic agents, care should be taken on the next step about reinitiation of ATT in such patients.
Earlier American Thoracic Society guidance (2006) recommends “bridge therapy” in patients with active tuberculosis, where hepatotoxic first line agents such as isoniazid, rifampin, and pyrazinamide are replaced with non-hepatotoxic second line alternatives such as fluoroquinolones, ethambutol, and aminoglycosides like Levofloxacin, with close monitoring of liver function test; however, this approach is not explicitly addressed in the 2016 updated American Thoracic Society guidelines.
After 3 weeks, transaminases normalized and he remains clinically stable, but sputum smear is still positive. What is the most appropriate next step in management?
A. Restart all first-line medications simultaneously at full dose with weekly liver enzyme monitoring
B. Reintroduce rifampin first with graded dosing, then isoniazid. Defer pyrazinamide unless immediately essential
C. Reintroduce isoniazid first because it has the highest early bactericidal activity
D. Permanently avoid all hepatotoxic medications and continue second-line regimen for 18 months
E. Perform liver biopsy before reintroducing any first-line agent
Answer: B
Reintroduction is done only after liver enzymes fall to <2 of upper limit normal and bilirubin normalizes, because restarting earlier increases the risk of recurrent and potentially fulminant liver injury.
Reintroduction of hepatotoxic first-line anti-tubercular drugs after resolution of DILI is recommended even in asymptomatic patients because the goal of tuberculosis treatment is microbiological cure and relapse prevention, not merely symptom control. Core agents such as rifampicin and isoniazid have the strongest bactericidal activity and are essential to achieve durable treatment success within the standard treatment duration. Non-hepatotoxic alternatives (e.g., ethambutol, fluoroquinolones, aminoglycosides) are generally used as temporary substitute regimens during hepatotoxicity but are less effective for clearance when used alone in drug-susceptible TB and typically require longer, more complex courses with higher risks of failure or resistance. Therefore, once liver function normalizes, hepatotoxic drugs are reintroduced sequentially with monitoring to restore an optimal curative regimen while identifying any specific offending agent if toxicity recurs.
Drugs are reintroduced one at a time so that the offending agent can be identified if transaminases rise again. The preferred sequence is rifampin first, since it has the most critical mycobactericidal activity and a moderate hepatotoxic risk, lower than pyrazinamide and comparable or slightly lower than isoniazid depending on cohort data. If liver tests remain stable after about one week, isoniazid is added next, followed by pyrazinamide last, as it carries the highest hepatotoxic potential and may be avoided entirely if the prior episode was severe (e.g., jaundice with coagulopathy or encephalopathy), with treatment extended to 9 months.
Some protocols use low-dose initiation for a few days before reaching full dose, but the key principle remains stepwise rechallenge with close LFT monitoring. Importantly, the effective duration of ATT is counted only after the full hepatotoxic regimen is successfully restarted, not during the interruption phase.
Counseling patients and their families is crucial when the primary regimen is reintroduced since anti-tubercular related side effects may result in non-adherence, potentially compromising tuberculosis management. Therefore, emphasis should be placed on the importance of anti-tubercular adherence while reassuring patients and parents about safety protocols, close monitoring, and stepwise reintroduction of therapy. Individualized selection of anti-tubercular drugs and careful adjustment of the treatment plan are key to balance the hepatotoxic risk with effective tuberculosis control. Failure to appropriately address these challenges may lead to treatment discontinuation or interruptions, both of which can lead to poor outcomes, including disease progression and the development of drug resistance.
Learning Points:
In the present scenario, the child is clinically asymptomatic, with no physical exam findings suggestive of chronic liver disease, and other causes of hepatitis have been excluded. This clinical situation addresses:
- How to diagnose a drug induced liver injury
- When to consider DILI in your differential for acute hepatitis
- The histopathologic appearance of DILI on a liver biopsy
- How to approach anti-tubercular therapy (ATT) related DILI, especially in the pediatric population