Why should we screen for hepatitis delta?

As trainees, we are well versed in screening for hepatitis B (HBV) and hepatitis C (HCV). However, few of us have experience with hepatitis delta (HDV). This post will offer a quick history and review of hepatitis D and remind us about why screening is so important!
HDV was first reported in humans in Italy in 1977 by Rizzetto in a cohort of Italian patients with HBV presenting with severe hepatitis. A new antigen, called the delta antigen, was detected by direct immunofluorescence in the liver cell nuclei of patients with HBsAg positive chronic liver disease, as seen in the following figure of immunofluorescence of post-mortem liver.
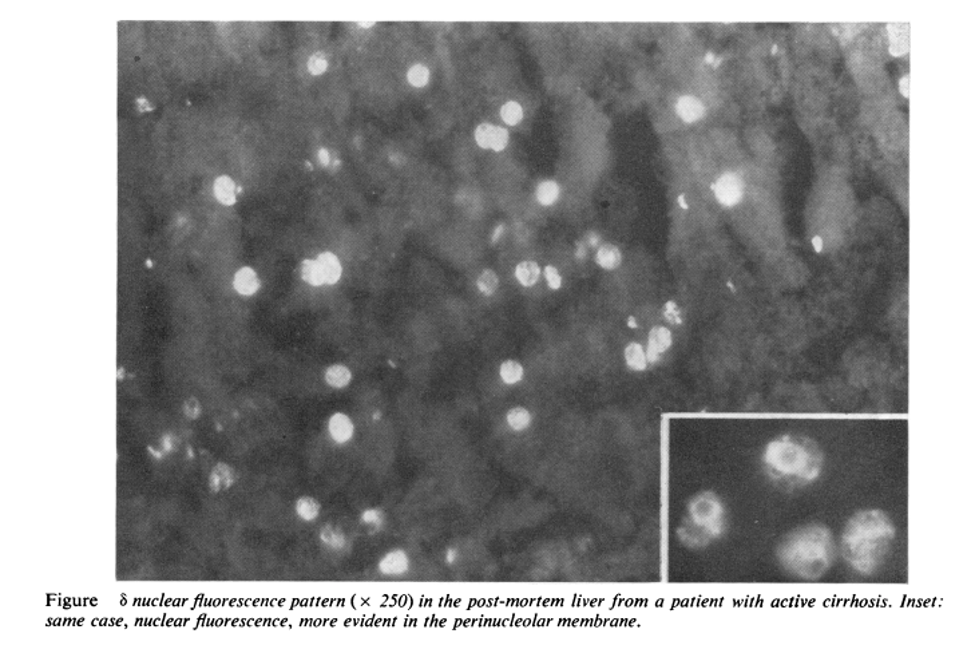
This delta antigen was found in higher prevalence in patients with HBsAg positivity with liver damage. This antigen was initially thought to be a newly identified antigen of HBV, however, after collaboration with the National Institute of Health and work in chimpanzees, it was soon found to be a “defective” virus that required the hepatitis B surface proteins for hepatocyte entry, with the HDAg encoded by small 1.7 kb single strand of ribonucleic acid (RNA).
What is the clinical course of Hepatitis D?
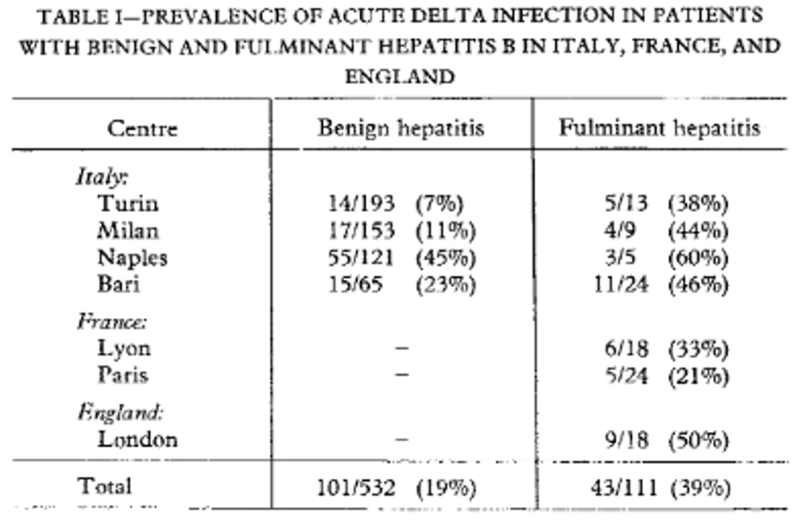
HDV infection occurs in one of two patterns, HBV-HDV co-infection and HDV superinfection. HBV-HDV co-infection occurs when infection with both viruses occur simultaneously. This pattern can result in extensive hepatic necrosis and can manifest with severe or fulminant hepatitis with a high case fatality rate. In a 1982 study that included 532 patients with “benign” HBV-HDV hepatitis and 111 patients with HBV-HDV fulminant hepatitis, the authors found that acute delta infection, defined by presence of the delta antigen or IgM anti-delta, was more frequently found in patients with fulminant hepatitis. These results are shown in the table below.
Recovery from HBV-HDV co-infection often results in clearance of both viruses, with an estimated 5% progressing to chronic HDV infection.
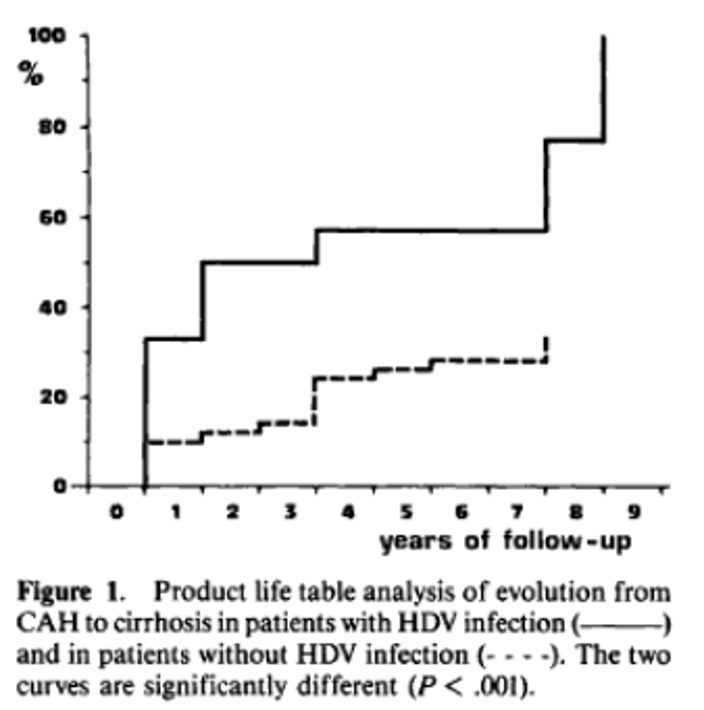
The other pattern of transmission is HDV superinfection, where patients with chronic HBV infection become infected with HDV. HDV superinfection frequently results in chronic HDV infection, which leads to accelerated progression to cirrhosis and an increased risk of HCC, compared to patients with chronic HBV mono-infection, with the following figure providing a visual timeline of the evolution from chronic active hepatitis to cirrhosis in patients with HDV infection compared to patients with HBV mono-infection.
How do we screen and diagnose Hepatitis D?
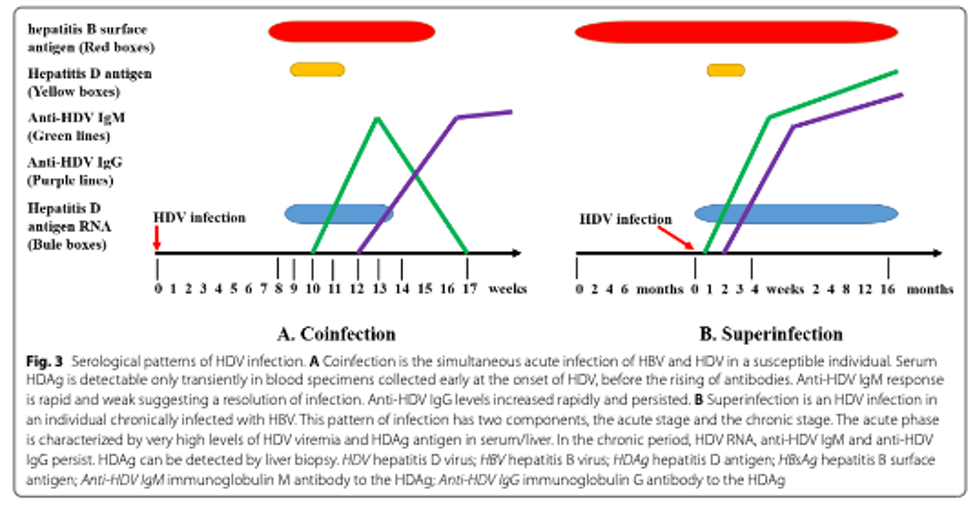
Screening for HDV with serological markers including anti-HDV IgG, IgM, and total antibody. IgM anti-HDV is detectable within 2-3 weeks of symptom onset and disappears about 2 months after an acute co-infection, but remains detectable in superinfections. HDV IgG and HDV total antibodies persist after the resolution of acute co-infection and in patients with chronic infection. A positive anti-HDV IgG or anti-HDV total Ab result suggests previous or ongoing exposure to HDAg. HD Antigen (HDAg) is detectible in serum for about 2 weeks and can also be detected on liver biopsy. A positive antibody result should be followed by a HDV RNA test to confirm ongoing viremia. In 2017, a World Health Organization international RNA standard was made available, allowing for reporting of results in international units. The serologic and RNA patterns of both HBV coinfection and superinfection are shown in the figure below.
While both screening and confirmatory testing have become more widely available, guidance on screening is variable. The 2017 European Association for the Study of the Liver (EASL) Guidelines and the 2016 Asian Pacific Associated for the Study of the Liver (APASL) clinical practice guidelines on management of chronic hepatitis B recommends systematic screening of all patients with HBsAg positivity for co-infections including HDV, HCV, and/or HIV. In contrast, the 2018 American Association for the Study of Liver Disease (AASLD) recommends screening patients for HDV only if they have HBV DNA <2,000 IU/mL but elevated ALT, or are at risk for HDV, which they define has having HIV and/or HCV infection, use of intravenous drugs, men who have sex with men, people with multiple sexual partners or any history of sexually transmitted infections, or are immigrants from areas with high HDV endemicity.
In the U.S., despite current professional guidance, screening for hepatitis D, is rarely performed. In fact, in a 2015 Veterans Affairs retrospective cohort study including 25,603 patients with HBsAg+ in the United States, only 8.5% of patients were tested for HDV with 3.4% of these patients testing positive. Only 6 (8.2%) of HDV-positive patients underwent confirmatory PCR testing. Receiving an HDV test was associated with testing for HBV, HIV and HCV. Patients with a high-risk profile (high-ALT, low HBV DNA) were more likely to be tested, however 1,181 of 1,468 (80%) of patients with this high-risk profile were not tested. Patients with alcohol use and HCV were less likely to be tested for HDV. Interestingly, the majority (59%) of HDV-positive patients were also HCV co-infected. Factors associated with HDV positivity included HCV Ab, substance use, cirrhosis, and a “high risk profile”, as seen in the following table.
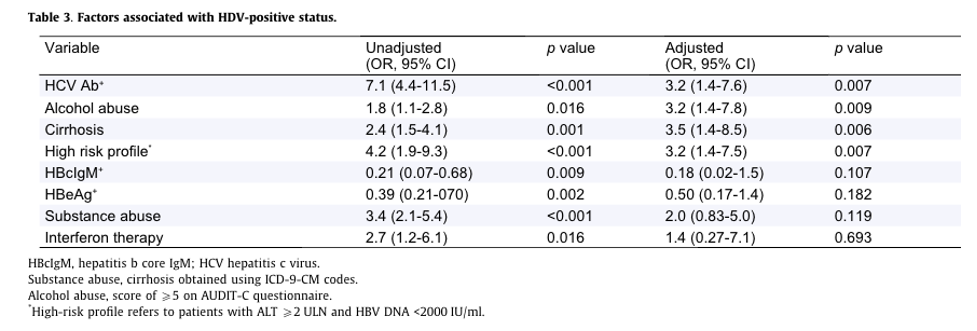
This study demonstrates low rates of HDV testing in the United States, even among patients with high-risk profiles.
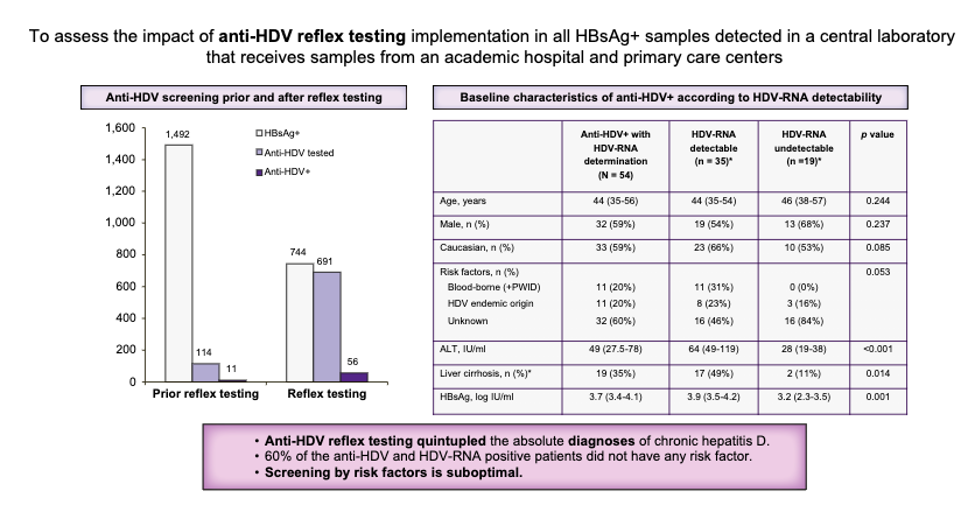
In Europe, where EASL recommends universal anti-HDV testing of all HBsAg-positive individuals, many cases still remain undiagnosed. A recently published study on the implementation of anti-HDV reflex testing among HBsAg-positive individuals including 2236 HBsAg samples found that using reflex testing led to a 5-fold increase in diagnosis of HDV infection. Prior to the implementation of reflex testing, only 7.6% of HBsAg-positive individuals were tested for anti-HDV. This study shows that the implementation of reflex HDV testing in HBsAg increases the diagnosis of patients with HBsAg, with the graphical abstract of this study below.
What is the prevalence of Hepatitis D?
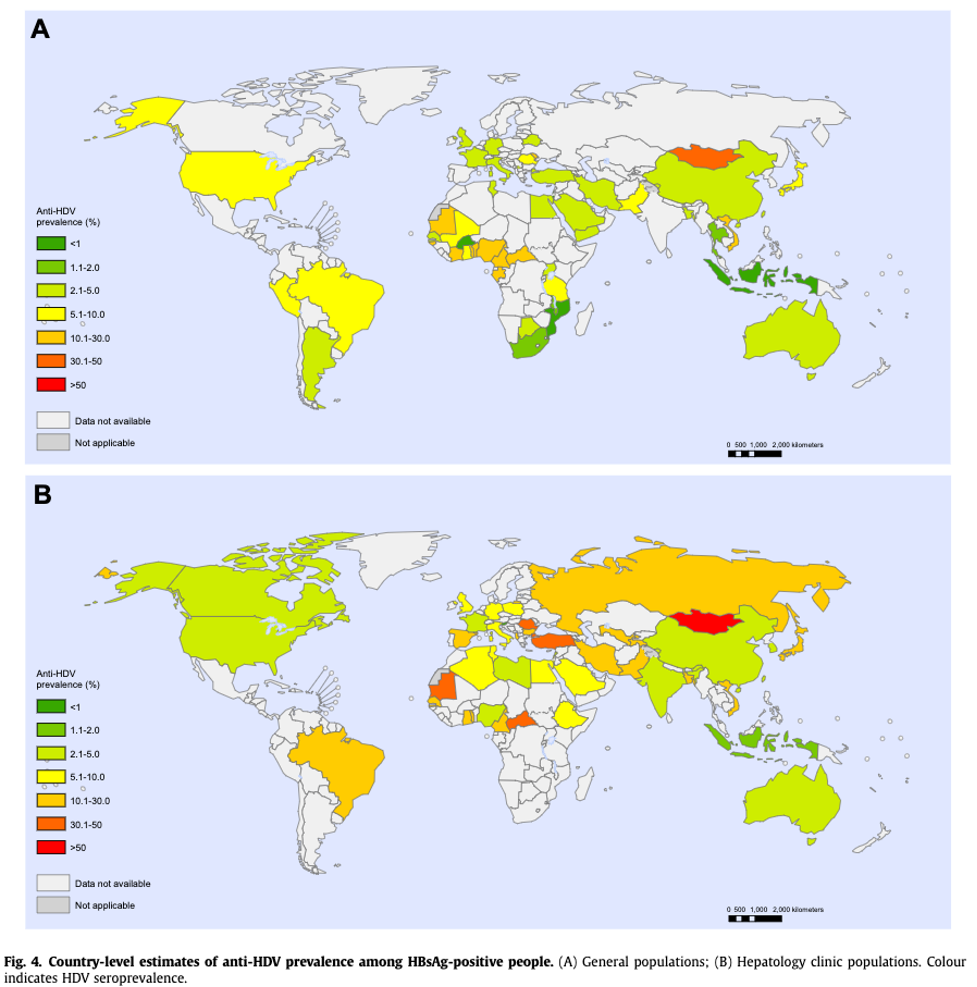
Global estimates of HDV vary widely, with recent estimates ranging between 12 and 74 million infections globally. Given the lack of universal screening of HBsAg-positive individuals for anti-HDV, the true prevalence of HDV infection is likely underestimated. The prevalence and geographic distribution of HDV have also changed over the last few decades with the implementation of Hepatitis B vaccinations, which first began in Europe and the United States in the early 1990s. With the implementation of HBV vaccination, the vaccinated population is no longer susceptible to HBV and therefore is also protected from HDV. Globally, the prevalence of HDV is quite variable, with data from many countries lacking. In a recent systematic review and metanalysis, the estimated global prevalence of HDV among HBSAg-positive people was 4.5%. The prevalence was highest in people who inject drugs or have HCV or HIV. HDV “hot spots” remain in Romania, Moldova, parts of Russia, Mongolia, Uzbekistan, Pakistan, Vietnam, areas of Africa, and the Amazon Basin of South America. The following figure from Stocktale’s systematic review and metanalysis offers a visual on country level estimates of HDV seroprevalence in the general population (A) and the hepatology clinic populations (B).
In the US, a 2019 study using the 2011-2016 National Health and Nutrition Examination Survey (NHANES) that included data from 16,143 adult participants, the estimated overall prevalence of HBsAg was 0.36%, with a prevalence of 3.4% in non-Hispanic Asians. Among the adult HBsAg+ population, 42% had antibodies to HDV, with anti-HDV prevalence of 46% in HBsAg foreign born adults versus 33% in US born adults. This study suggested a much higher prevalence of HDV than previously thought. In contrast, a NHANES study using data from 1999-2012 that included 52,209 individuals with HbsAg and HB core antibody found an overall prevalence of HDV of just 0.02% (10/52,209). The discrepancy between these two studies may be because this was the first NHANES analysis of HBsAg and ant-HDV to use data in which Asians were over sampled, with HBV and HDV endemic in several Asian countries.
How do we treat HDV?
Unfortunately, there is no approved treatments for HDV. While AASLD, EASL, APASL recommend pegylated interferon for HDV, interferon is not FDA approved for treatment of HDV. Interferon-alpha was first studied in 1986 in 11 patients in Italy, with a high recurrence rate after treatment discontinuation (4 of 6 patients). However, high doses of interferon-alpha do have a benefit in long-term clinical outcomes. In a follow up study of a RCT where patients were treated for 48 weeks with varying doses interferon alpha, patients who received high doses of treatment had significantly improved long-term survival when compared to the low-dose and the untreated controls, as seen in the Kaplan-Meier curve below.
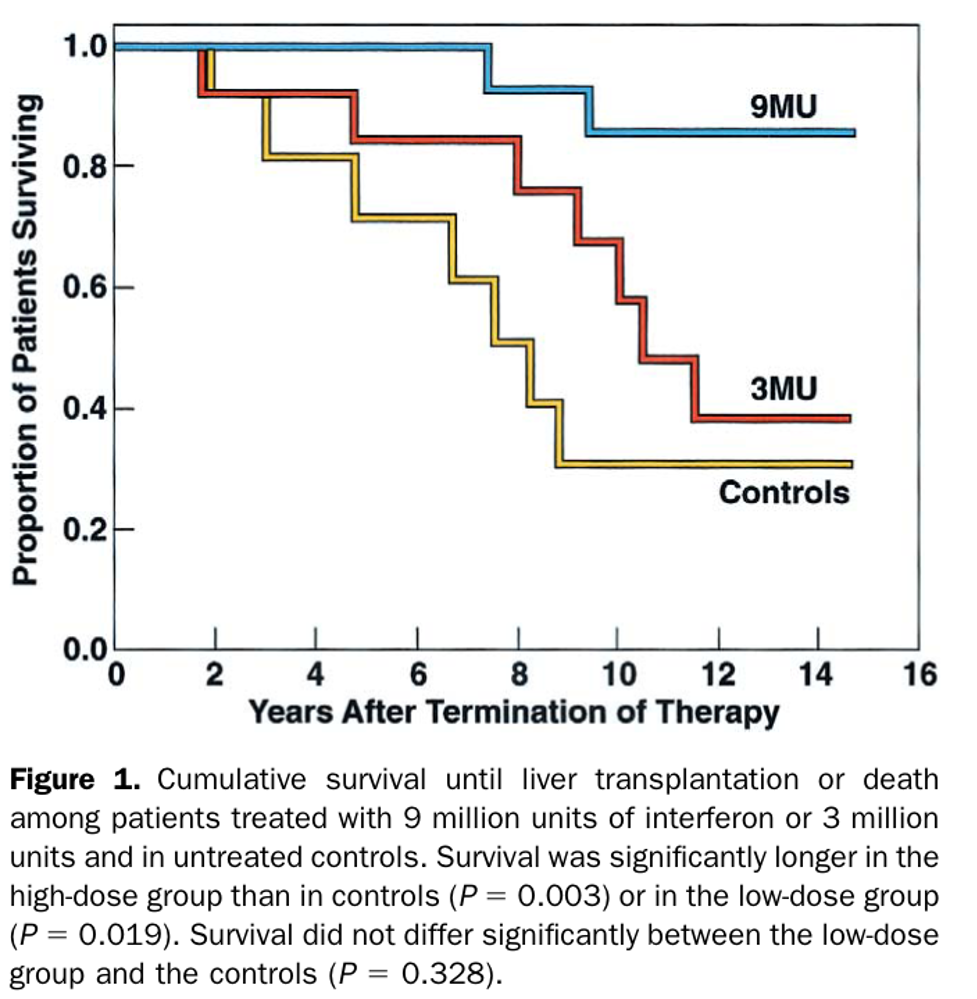
Furthermore, patients treated with high doses had a sustained decrease in HDV replication and an improvement in liver histology and fibrosis, even in the presence of cirrhosis (though only Childs-Pugh class A were included in the initial trial). While interferon-alpha certainly has a benefit, sustained viral response remains low and the recurrence rate after stopping therapy is high. Furthermore, interferon has significant adverse effects and a narrow therapeutic window in patients with cirrhosis, which further limits its use.
Thankfully, over the last several years, new treatments have been developed, including bulevirtide, an entry inhibitor that was recently granted conditional approval by the European Medicines Agency, and lonafarnib, which is currently being studied in a phase III clinical trial. Bulevirtide has the benefit that it can be used safely in patients with cirrhosis with contraindications to interferon.
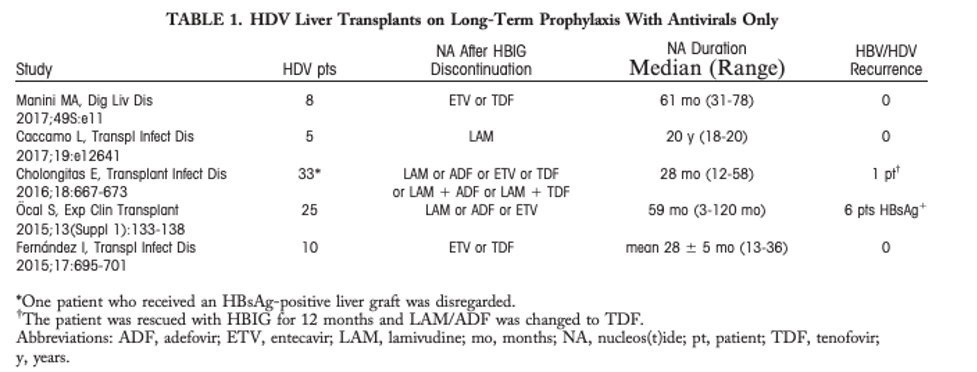
Liver transplantation is the only treatment option for end-stage liver disease due to HDV. While the rate of reinfection is lower in HDV than HBV due to the need for HBV to reestablish infection in the liver graft to drive expression of HDV, HDV recurrence is high. In the first series of transplantation for HDV cirrhosis, 70% of patients were found to have HD-Ag in the graft. In another case series, 18% of patients cleared both HBV and HDV after transplant, however HDV reinfection occurred in over 80% of patients, with an overall 77.7%. These early studies led to the use of HBV Immunoglobin (HBIg) to suppress HBV in this patient populations. With the development of nuleoside analogs (NA) against HBV, the combination of HBIg and NA as a prophylaxis regimen results in HBV-HDV reinfection rates of less than 5%. Given that HBIg is expensive and somewhat cumbersome to administer, NA monotherapy for prophylaxis is under study, with promising results. The table below from a letter to the editor summarizes HBV/HDV recurrence of HBV/HDV infection after transplant in patients receiving only NA therapy.
Closing thoughts
Given that HBV-HDV co-infection results in accelerated liver disease with poor outcomes and no approved treatments currently available, HDV continues to pose a significant public health risk. Thus, it is imperative that we screen patients at risk of HBV-HDV co-infection per AASLD guidelines. It is also important for the global hepatology community to agree upon a screening approach to obtain a more accurate understanding of global prevalence so that resources can be properly allocated once effective therapies become available.